

Why this topic needs a careful reset
A proper regenerative medicine Thailand dialogue presents information in such a way that it slows the audience down not speeds them up. It should inform precisely which cell type is the focus, if the method discussed has undergone a clinical trial, what end point measures are employed or how much remain uncharacterized. According to the FDA, regenerative medicine therapies have not been authorized for use in autism and that is why ISSCR produced its patient guide —to help educate patients and families on how they can ask better questions about stem cell treatments or clinical trials prior to thinking any way more than availability equals validity.
What “Natural Cellular Regeneration” means in alopecia areata
The follicle is not dead — but it is under immune attack
The phrase Natural Cellular Regeneration seems to pop up around alopecia areata for one key reason: the condition is rare; in many cases, the follicle isn’t so far gone that it can’t be salvaged. However, instead of disrupted by viruses it is functionally affected with immune activity. This biological possibility makes spontaneous regrowth possible in some individuals and potentially explains why hair growth can sometimes resume after treatment. However, this does not mean they have cured the disease or permanently reset follicle environment. The autoimmune process itself remains unpredictable, often relapsing.
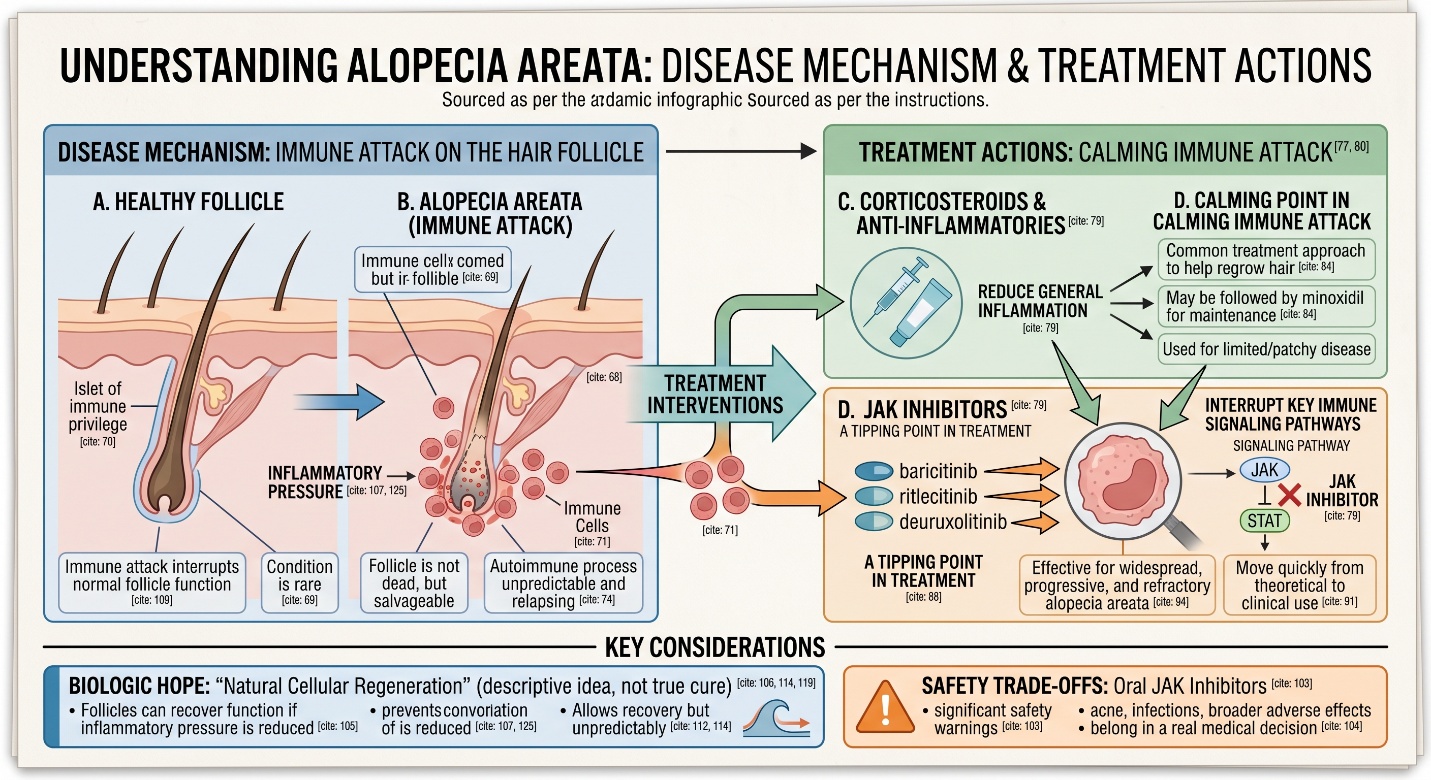
“Regeneration” is only part of the story
This is the first layer that matters. In alopecia areata, regrowth is not just about stimulating the follicle. It is also about calming the immune process that is disrupting it. That is why the most effective modern therapies are not marketed primarily as “regenerative” agents. They are immune-targeting treatments, especially JAK inhibitors, corticosteroids, and other anti-inflammatory approaches selected according to age, disease extent, and severity. In other words, Natural Cellular Regeneration sounds appealing, but in alopecia areata the practical medical question is usually: how do we stop the immune attack long enough for the follicle to recover?
Alopecia treatments that work: what actually has evidence
For limited patchy disease, corticosteroids still matter
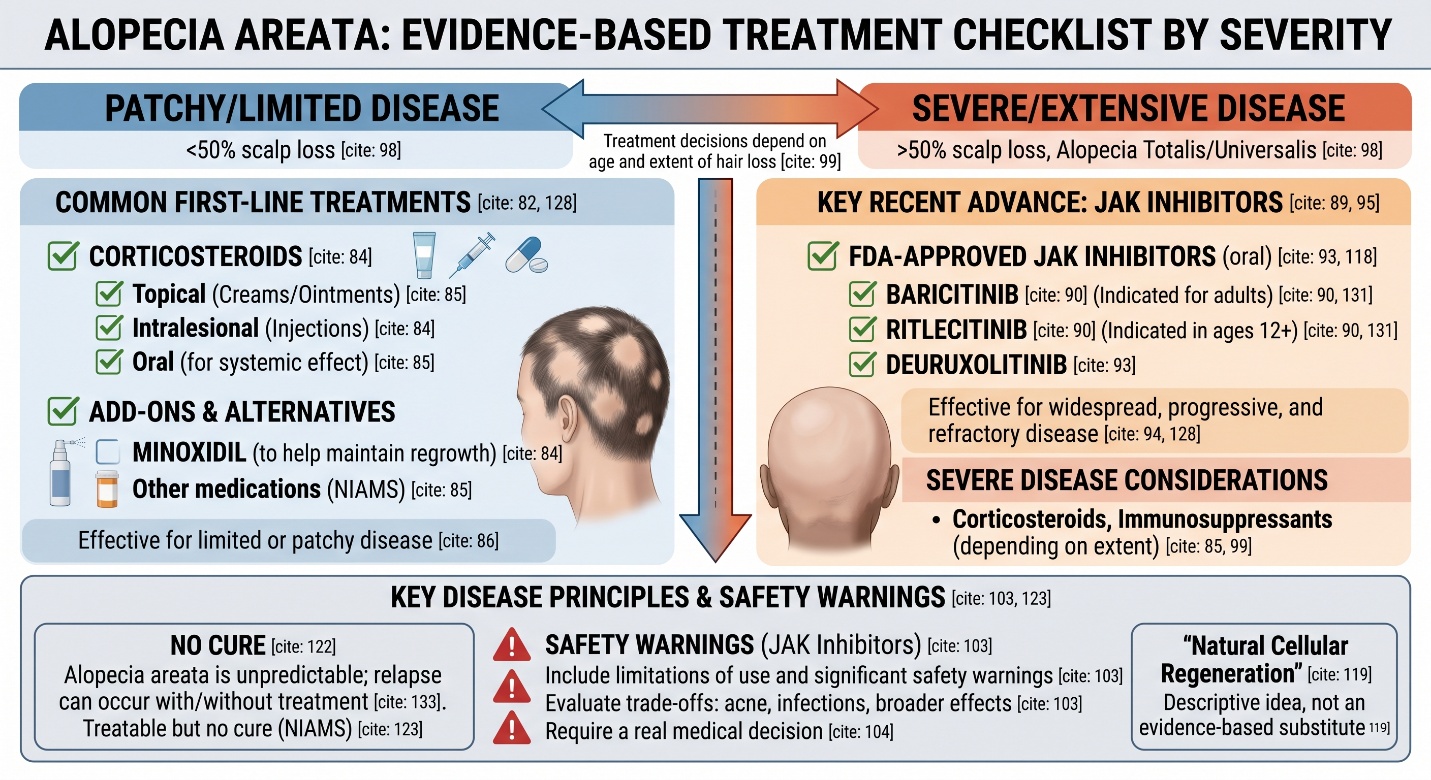
A lot of SEO content jumps straight to “breakthroughs,” but everyday dermatology still matters here. The American Academy of Dermatology says a common treatment approach for alopecia areata includes corticosteroids to help regrow hair, sometimes followed by minoxidil to help maintain regrowth. NIAMS also lists corticosteroids, immunosuppressants, and other medications that may be used depending on age and extent of hair loss. That may sound less futuristic than people expect, but these remain part of the real answer to alopecia treatments that work, especially when the disease is limited or patchy rather than severe and extensive.
For severe disease, JAK inhibitors changed the landscape
This is where the tipping point for the field emerged. JAK inhibitors have recently been said to change the game in severe alopecia areata treatment as outlined by recent reviews. Baricitinib: FDA approved for adults with severe alopecia areata (2022), and ritlecitinib was recently reviewed by the FDA, and is indicated in ages 12 and older with moderate to severe alopecia areata. This class moved quickly from theoretical to clinical use with a 2024 European expert consensus identifying baricitinib and ritlecitinib as the only two EMA-approved treatment options available at that time for alopecia areata.
The JAK story kept moving in 2024 and 2025
The treatment landscape did not stop there. A 2025 review of current and emerging JAK inhibitors states that recent clinical advances have led to FDA approval of three JAK inhibitors for alopecia areata: baricitinib, ritlecitinib, and deuruxolitinib. The same review notes durable efficacy signals for baricitinib, while other recent reviews conclude that JAK inhibitors are effective treatments for widespread, progressive, and refractory alopecia areata. This is probably the strongest current answer to the SEO phrase alopecia treatments that work when the disease is severe.
What works best depends on the kind of alopecia areata
Mild and localized disease is not the same as severe disease
This is the second layer that people miss, patchy scalp loss compared to widespread, or alopecia totalis versus auto-immune alopaecia universalis. Treatment decisions depend on age and extent of hair loss, states the National Institute of Arthritis & Musculoskeletal and Skin Diseases (NIAMS), while such distinction with respect to how dermatologists approach younger children compared to older ones is also reflected by a further breakdown made by the AAD into limited patchy disease or more extensive involvement. And when somebody asks for what alopecia treatments work, the most honest response possible is never black and white.
Severity changes the risk-benefit discussion
That matters especially with systemic JAK inhibitors. These treatments are important advances, but they are not casual beauty products. FDA labeling for baricitinib and ritlecitinib includes limitations of use and significant safety warnings, and recent safety reviews of oral JAK inhibitors continue to evaluate trade-offs such as acne, infections, and broader class-related adverse effects. So yes, these drugs are among the most important alopecia treatments that work for severe disease — but they also belong in a real medical decision, not just a keyword list.
Where “Natural Cellular Regeneration” fits — and where it does not
It makes more sense as a biologic hope than as a formal treatment class
The phrase Natural Cellular Regeneration works well as a way to explain why alopecia areata can be reversible in some people: the follicle is often still there, and regrowth can occur when inflammatory pressure is reduced. But it is not a guideline-defined treatment category, and it should not be allowed to blur the actual mechanism of the disease. The strongest current therapies for alopecia areata work not because they magically “rejuvenate” hair, but because they help interrupt the immune process that keeps follicles from functioning normally.
The honest version is better than the romantic version
This is probably the most useful way to say it. Alopecia areata is one of those conditions where regrowth can happen, but unpredictably. That unpredictability is exactly why people are drawn to words like “regeneration.” Still, the stronger, more honest version of the story is this: the biology allows recovery, but medicine usually works by modulating immune disruption rather than by offering a true cure. That distinction may sound less dramatic, but it is much closer to what patients actually need to hear.
The most honest conclusion
If someone asks what currently defines alopecia treatments that work, the answer is clearer today than it was a few years ago. For limited disease, corticosteroid-based strategies remain important. For severe alopecia areata, JAK inhibitors have changed the standard conversation in a very real way. But Natural Cellular Regeneration should still be treated as a descriptive idea, not a substitute for evidence. In alopecia areata, the most believable progress has come from understanding the immune biology of the disease and targeting that biology directly.
Frequently Asked Questions
1) Is there a cure for alopecia areata?
No. NIAMS states that there is no cure for alopecia areata, although there are treatments that can help hair grow back more quickly.
2) What does “Natural Cellular Regeneration” mean in alopecia areata?
It is best understood as the idea that hair follicles may recover function if the immune disruption around them is reduced. It is not a formal medical treatment category.
3) Which alopecia treatments that work are most evidence-based right now?
For patchy disease, corticosteroid-based approaches remain important. For severe disease, JAK inhibitors such as baricitinib, ritlecitinib, and now deuruxolitinib have become the biggest evidence-based advance.
4) Are JAK inhibitors approved for everyone with alopecia areata?
No. Approval depends on the specific drug and patient age. Baricitinib is approved for adults with severe alopecia areata, while ritlecitinib is approved for adults and adolescents aged 12 and older with severe alopecia areata.
5) Does hair regrowth mean the disease is gone for good?
Not necessarily. Alopecia areata is unpredictable, and regrowth can occur with or without treatment, but relapse can also happen. That is one reason ongoing medical follow-up still matters.