

Parkinsons disease is an incurable degenerative neurological disorder that impacts the movement, balance, coordination, sleep,mood, digestion, speech and independence on daily basis. The thing I find most debilitating about Parkinsons for many patients and families is that it is not only the tremor or stiffness, but rather than slow loss of quality of life, confidence, mobility and long term function.
Current care in Parkinson’s disease is mainly geared toward symptom control, particularly with dopaminergic medication as well as rehabilitation, exercise, nutrition support and neurological monitoring. These approaches remain essential. But since certain biological processes such as neuroinflammation, oxidative stress, mitochondrial dysfunction, α-synuclein pathology or immune dysregulation and problems with protein clearance are involved in the pathogenesis of Parkinson’s disease some patients before supportive regenerative strategies like Stem Cell and DFPP for Parkinson’s Disease. Recent narratives note that Parkinson disease is a multisystem disorder driven by biological mechanisms in both the CNS and peripheral systems rather than solely caused by dopamine loss.
For a medically appropriate explanation of this, it is not complicated at all: DFPP can prepare the inner biological milieu first, and then UC-MSCs may play a supportive role via paracrine and immunomodulatory signaling. This should not be termed a cure nor a substitute for traditional neurologic therapy.
What Is DFPP?
Double Filtration Plasmapheresis (DFPP) is a blood purification method in which plasma is separated and filtered to remove certain larger circulating elements. There is only clinical literature regarding DFPP in selected medical contexts—DFPP reduces high-molecular-weight plasma components, such as immune complexes, immunoglobulins, lipoproteins and inflammatory-related factors.
DFPP should not be promoted as a comorbidity treatment for Parkinson’s disease. It may then be considered as a biological preparation phase before fill in UC-MSCs.
A patient-friendly explanation would be:
In this context, DFPP may be a solution to decrease some undesirable systemic load circulating in the bloodstream, paving the way for a cleaner and balanced internal milieu that precedes UC-MSC administration.
What Are UC-MSCs?
Umbilical cord-derived mesenchymal stromal/stem cells (UC-MSCs) have been widely studied in regenerative medicine, primarily due to their limited “pathological memory” and ability to secrete bioactive molecules, extracellular vesicles (EVs), cytokines, growth factors and other paracrine signals. These cells are typically not perceived as simple “replacement cells” for neurons that produce dopamine lost through the course of degeneration. In particular, their potential value is often associated with immune modulation, inflammatory balance, trophic signaling and tissue microenvironment support. As nonspecialists, reviews of MSCs in Parkinsons disease outline multiple possible mechanisms (immunomodulatory effects, neurotrophic support, anti-inflammatory communication, and extracellular vesicle activity) whilst cautioning on how the clinical evidence remains limited.
For patients, this translated into the aim not being to “provide overnight brain cell replacement.”. A more accurate concept is:
One possibility is that UC-MSCs would be involved through signaling mechanisms to support the biological environment surrounding damaged or stressed tissue.
Table of contents Why Combine DFPP Before UC-MSCs for Parkinson Disease?
The concept of Stem Cell and DFPP for Parkinsons disease is biological preparation.
If the bloodstream is high in inflammatory mediators, abnormal lipid-related particles, immune complexes, oxidative stress signals or other non-optimal circulatory burden then perhaps the internal signaling environment of the body is not up to scratch. Within this concept, DFPP could be first used to eliminate certain circulating factors. Then UC-MSCs could be applied into more suitable biological settings.
This can be understood through the letter of soils and seeds that explains
DFPP helps prepare the soil, UC-MSCs provide biological signaling support.
This is not to say DFPP will give stronger stem cell effects. Semantic analysis suggests that DFPP may be construed as a pre-conditioning strategy which plays a role to optimise the internal milieu before cellular-based support.
Stem Cell and DFPP for Parkinson Disease: Possible Advantages in Patients
Prepares the Body Ahead of UC-MSCs
Perhaps the most clinically significant advantage of DFPP is that it may be beneficial in alleviating selected circulating burden prior to administration of UC-MSCs. This may include some immune complexes, inflammatory-related factors and lipid-associated factors.
For the patients, it adds some structure to the program:
Assessment → DFPP preparation → UC-MSCs support → rehabilitation → follow-up
This approach is more useful than offering UC-MSCs alone as a single prescription.
Helps Support a Balanced Inflammatory Response
More and more, inflammation is talked about as a key component of Parkinson’s disease biology. Utilising neuroinflammation, systemic immune activation, oxidative stress and mitochondrial dysfunction as a pathophysiological framework to explain the progression of disease and symptoms burdened.
Conclusions: DFPP may decrease some circulating factors related to inflammation. This UC-MSCs could then be used due to its proposed immunomodulatory and anti-inflammatory signaling capabilities.
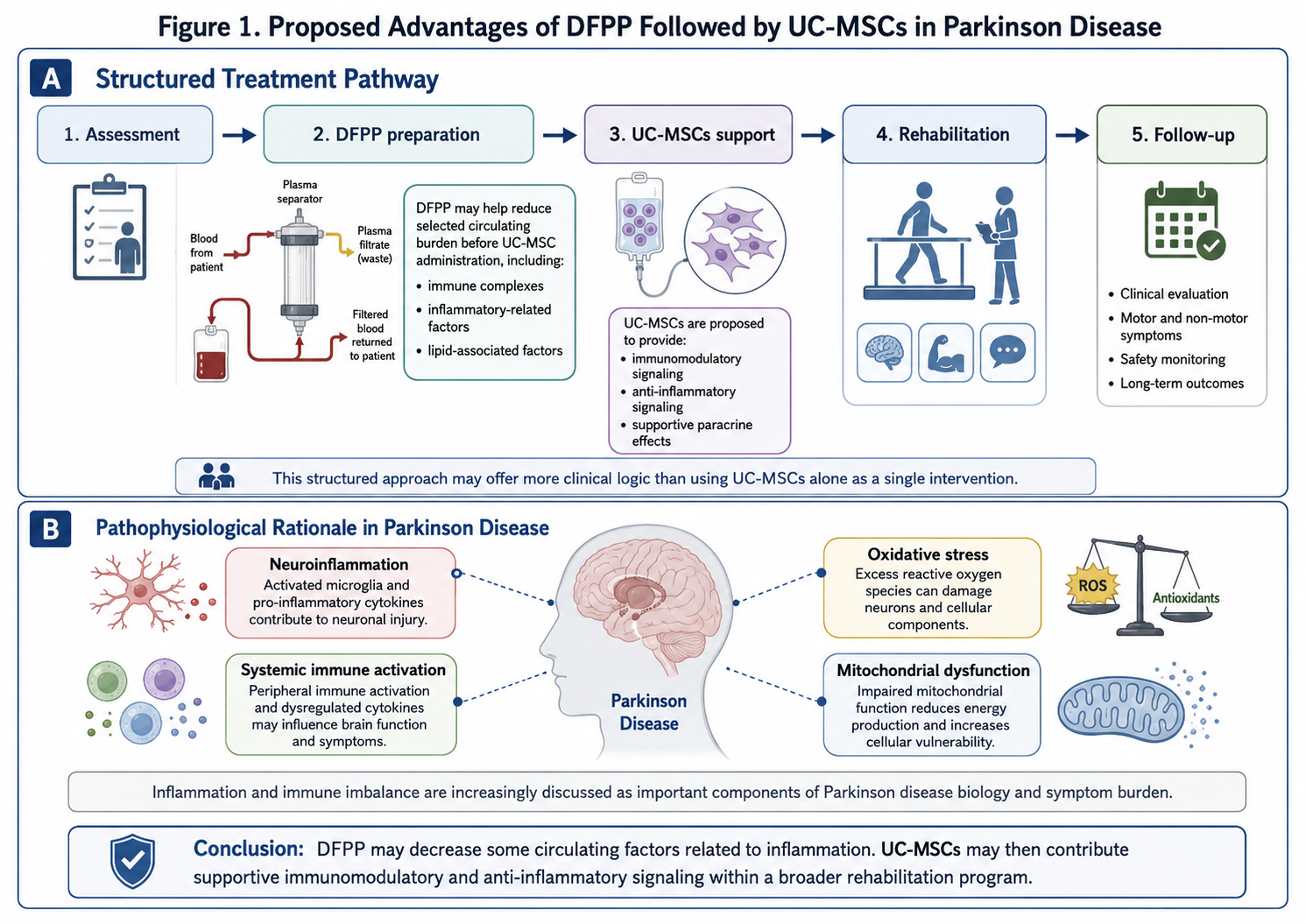
Figure 1: Proposed Treatment Pathway Combining DFPP and UC-MSCs for Parkinson Disease
An example of a more cautious medical statement would be:
DFPP and UC-MSCs may promote inflammatory equilibrium in select PD patients but should not be heralded as halting disease progression.
May Support the Biological Microenvironment
There are many things that at play, Parkinsons is not one pathway. These include dopaminergic neuronal stress, α-synuclein aggregation, mitochondrial dysfunction, oxidative damage, neuroimmune dysregulation and gut–brain axis involvement.
Due to this complexity, a nurturing regenerative program should not be focused on alleviating just one symptom. It will be more appropriate to assist wider biological microenvironment.
Choice of UC-MSCs may arise for hypothesized mechanisms by which they release signaling molecules that act on neighboring vascular cells, immune cells and tissue-supportive pathways. This may involve patients needing a wider supportive measure alongside standard medical care.
Complements Rehabilitation and Neurological Care
In the case of Parkinsons, no amount of regenerative support on their own, combining most of:
Neurologist-guided medication
Physical therapy
Balance and gait training
Strength and mobility exercises
Occupational therapy
Assistance with speech and swallowing as required
Nutrition and sleep optimization
Long-term symptom monitoring
More importantly, Stem Cell and DFPP programs should be utilized as a supportive adjunct – rather than an alternative to these foundations.
A patient-centered message is:
Perhaps the biology is supported by UC-MSCs, while rehabilitation serves as a bridge to movement, balance, confidence and function.
Increases the Individualization of Parkinson’s Disease Support Programs
Every Parkinson’s patient is different. Some patients mainly experience tremor. Some have more trouble with rigidity, bradykinesia, instability, fatigue, dysregulation of sleeping or bowel habits or fluctuations in the medication.
A comprehensive Stem Cell and DFPP for Parkinsons disease assured program should begin with Review:
Diagnosis and disease stage
Medication history
Motor symptoms
Non-motor symptoms
Sleep quality
Balance and fall risk
Mobility level
Cognitive and emotional status
Inflammatory or metabolic markers
General health and safety risks
This allows the program to be tailored and risk-neutral for the patient.
What the Program May Include
Medical and Neurological Assessment
Before creating a treatment plan, the practitioner should go over the patient’s medical history; Parkinson’s disease stage; and current medications as well as mobility, balance, sleep, mood and digestion issues; and general health.
DFPP Biological Preparation
DFPP potentially should be used as a pre-treatment modality to prevent certain circulating burden and facilitate a cleaner internal milieu prior to administering UC-MSCs.
UC-MSCs Administration
UC-MSCs may be applied by a medically-chosen path depending on the patient circumstance and medical doctor evaluation. It should be presented as investigational and supportive.
Rehabilitation Support
Therapies that support mobility and balance, such as physical therapy and occupational therapy, are often used to support potential functional outcomes.
Progress Monitoring
Patients and their families should track realistic results such as:
Walking stability
Balance confidence
Tremor severity
Muscle stiffness
Fatigue
Sleep quality
Daily activity tolerance
Mood and motivation
Medication response pattern
Quality of life
Important Medical Positioning
Stem cell products for neurological disease, including Parkinsons, are generally not approved by the U.S. FDA as an accepted treatment. Regenerative medicine products such as stem cells, exosomes, etc. rarely enter into clinical practice without FDA approval As discussed before innapropriate usage of these medical modalities as allowed by the FDS is warned to patients.
Consequently, the safest and most credible form of wording is:
Medically supervised informational and investigational program on potential treatment(s) Stem Cell and DFPP for Parkinsons disease. When, but not ever presented as a treatment, not replace Parkinson’s medications and should be undertaken in conjunction with supervision and care from an practicing neurologist.
Closing
For patients are considering options such as Stem Cell and DFPP for PKD, the best way to think of this whole program is a form of biological support or part of supportive care but not a cure. DFPP could potentially priming the body by decreasing certain circulating inflammatory, immune, and lipid-related burden prior to infusion of UC-MSCs. UC-MSCs may thus deliver supportive paracrine, immunomodulatory and antiinflammatory signals that may begin to develop a more amenable microenvironment.
Although this needs further clinical confirmation and the outcomes might not be uniform, a carefully structured program integrating biological preconditioning, supportive therapy with UC-MSCs, rehabilitation treatment as well as neurological monitoring offers promise in optimising patient outcomes with realistic treatment goals. For Parkinson disease, the optimal care remains integrated: traditional neurology, movement rehabilitation, patient safety and an appropriate view on regenerative medicine.