

Systemic lupus erythematosus (SLE) is a chronic autoimmune disease characterized by systemic inflammation and immunological dysfunction resulting in robust autoantibody production. Even with significant improvement over the past few decades, some patients remain refractory to conventional therapy, this is simply the reality in the current era of immunosuppressive therapies. Recent years have seen the evaluation of umbilical cord-derived mesenchymal stromal/stem cells (UC-MSCs) and double-filtration plasmapheresis (DFPP) as new therapeutic strategies for age-related diseases and other therapeutic areas owing to their immune modulation properties. Here, we highlight the biological rationale of using this combination and summarize preclinical and clinical evidence and limitation toward translating UC-MSCs with DFPP to SLE therapy. Both have been previously demonstrated to have underlying clinical activity but as a combination regimen are still being investigated for validation.
Introduction
Systemic Lupus Erythematosus (SLE) is a multifactorial disease characterized by loss of immune tolerance, autoantibody production and chronic tissue inflammation with multi-organ involvement, which most prominently affections the kidneys, skin, joints and central nervous system. Current standard therapy comprises long-standing traditional corticosteroids, the use of also immunosuppressive agents and biologic agents to achieve disease control while preserving organ function. SLE with active disease despite the provision of optimal medical therapy.
The pathophysiology of SLE ocular manifestations and therapeutic targets
Misdirected immune attention: Clinical perspective SLE is traditionally considered a disorder of immune deregulation, defined by
Dyshelperfunctionals and autoantibody (e.g. anti-dsDNA) generation
Dysregulated T-cell responses
Total, pro-inflammatory cytokine ( IL-6, IFN-α ) secretion
Tissue with immune complex deposits that causes chronic injury
Such pro-inflammatory pathways are associated with chronic inflammation and organ damage in lupus nephritis. Given this negative immunopathology, strategies that are able to re-balance the immune response rather than blunt it is especially attractive.
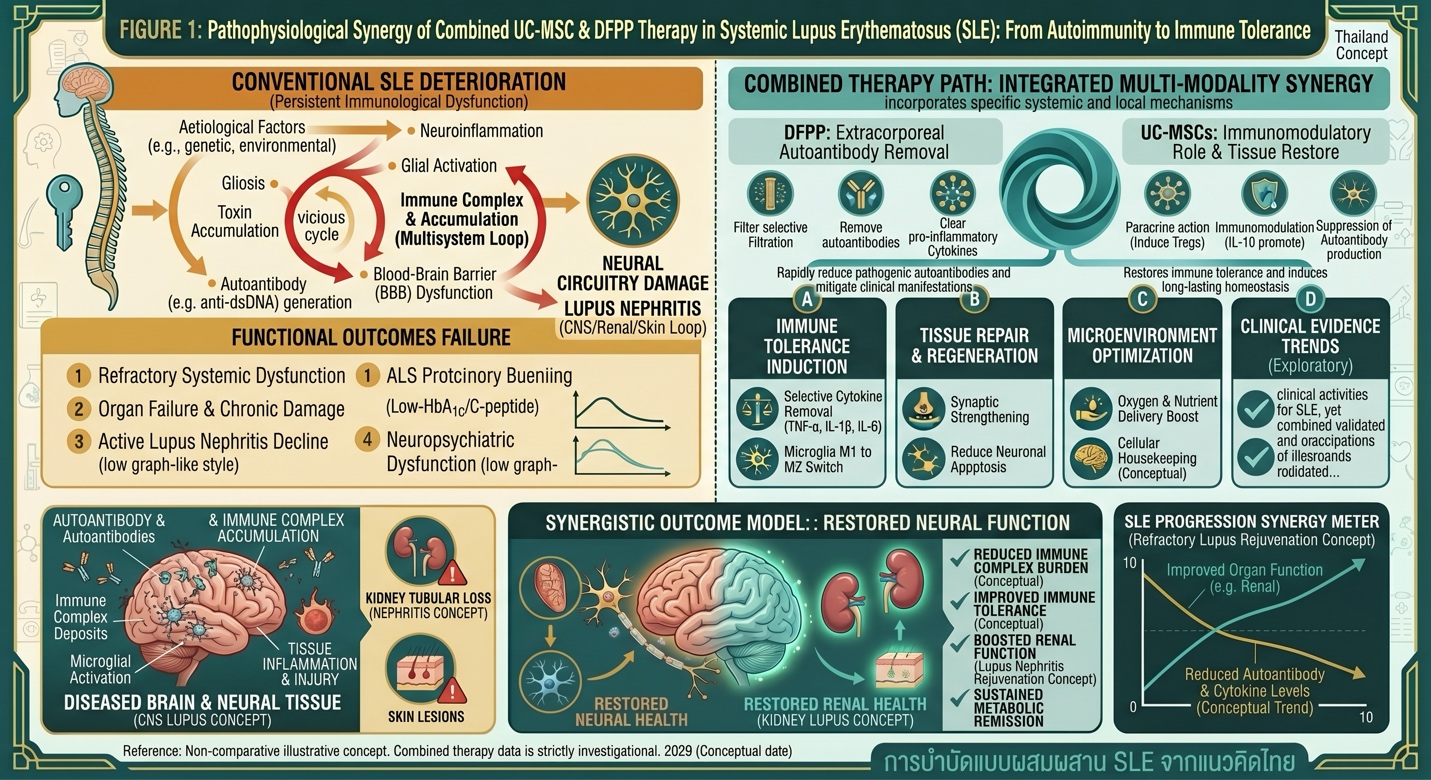
Figure 1: Schematic Comparison of SLE Pathological Progression vs. Integrated DFPP & UC-MSC Therapy, illustrating the dual mechanisms of autoantibody removal from circulation and induction of cellular immune tolerance
UC-MSCs: Immunomodulatory Role in SLE
Distinctive immunoregulatory and anti-inflammatory properties of UC-MSCs have opened new avenues towards exploring their potential utilization as a therapy for autoimmune diseases.
Key mechanisms include:
Diminution of autoreactive T and B lymphocytes
Induction of regulatory T cells (Tregs)
Reduction of pro-inflammatory cytokines
Suppression of autoantibody production
Secretion of trophic and anti-inflammatory factors in a paracrine fashion
The results of previous clinical studies of SLE have shown the efficacy and potential benefits. An illustrative one from a trial involving IV administration of UC-MSCs to unresponsive SLE patients is detailed as:
Reduction in disease activity scores
Regular improvements of lupus nephritis for renal function
Decrease in autoantibody levels
Similar studies have also demonstrated acceptable safety, however long-term efficacy and durability are still being determined.
Double-Filtration Plasmapheresis (DFPP): Mechanistic Basis
DFPP is a form of therapeutic apheresis that allows for the selective removal of high-molecular weight plasma components, for example:
Autoantibodies
Immune complexes
Inflammatory mediators
DFPP selective removal reduces centesis and repletion of fluid from peripheral spaces, compared to traditional plasma exchange.
In SLE, DFPP may help:
Rapidly reduce circulating pathogenic autoantibodies
Decrease immune complex burden
Distilled Control of disease activity. Indicated during acute or exacerbation events related to clinical status.
Temporary stabilization in refractory scenarios
Although DFPP has been applied in aggressive lupus nephritis and other autoimmune diseases following the immunosuppressive drugs originally used, especially in situations that require rapid immunomodulation needing continuous therapy.
Introduction to Application of Mechanism of Combined Therapy with UC-MSC and DFPP
Combination therapy with UC-MSCs + DFPP adherence to a complementary therapeutic premise:
Treating patients with DFPP has several advantages including, among others, the reduction of autoantibodies and circulating immune complexes from plasma.
That is as follows: UC- MSCs will restores the immune environment which ultimately lead to restoring of immunological homeostasis.
This dual approach may theoretically:
Improve the inflammatory microenvironment
Enhance responsiveness to cell-based therapy
Offer rapid and long-lasting immunomodulation
While exploratory in its clinical validation, the combination strategy has biologic plausibility.
Clinical Evidence and Current Limitations
MSC Therapeutics for Refractory Systemic Lupus Erythematosus, The majority of MSC therapy trials in refractory SLE have been conducted in China and Europe. These studies suggest:
Of clinical remission or partial response based on patient characteristics
Improvement in lupus nephritis outcomes
Reduced reliance on high-dose corticosteroids
However, limitations include:
Small sample sizes
Lack of standardized protocols
Variable follow-up duration
Limited randomized controlled trials
DFPP in SLE
In SLE, especially in severe cases, DFPP reduces autoantibodies quickly and mitigates clinical manifestation of the disease. Bridge therapy— not meant for the long term
Combination Therapy
Nevertheless, high-quality evidence has only evaluated the association of UC-MSCs with DFPP in SLE. Much of the data comes from small observational trials or extrapolated single modalities
And this is exactly why we must consider this hybrid approach as:
Promising but investigational
Part of the process for making clinical practice more consistent
Requiring further controlled studies
Safety and Regulatory Considerations
Good safety data have been recorded for both UC-MSC therapy and DFPP in controlled environments. However, considerations include:
Immune or infection risk
Cell quality and preparation variability
Need for regulatory oversight
International recommendations state that stem cell therapies should ensure quality, safety and efficacy standards in order to maximize the benefit and minimize the risk within a suitable clinical setting.
Clinical Implications and Patient Selection
Indications of UC-MSCs with DFPP in SLE.
Patients with refractory disease
A large percentage of cases with extensive organ involvement (such as lupus nephritis)
Situations requiring rapid immunomodulation
However, treatment should be:
Individualized
Supervised by experienced clinicians
Integrated with standard immunosuppressive therapy
Conclusion
The co-targeting of UC-MSCs and DFPP on SLE is an innovative one in both regenerative & immunomodulatory medicine. This approach is consistent with a recently gained understanding of SLE pathophysiology that combines targeting both systemic immune dysregulation and inflammatory burden.
Although the data in support of safety and possible effectiveness of each modality is still early, there are no data on combined therapy. ConclusionThese findings are grounds for future randomised controlled trials to investigate optimal regimens and outcomes.
For now, this methodology can be considered investigational in nature with proper patient selection and expectations.