

Pulmonary Crisis
Severe lung inflammation is a serious global health problem. Patients in respiratory failure must have emergency treatment to avoid death. Acute Respiratory Distress Syndrome (ARDS) causes diffuse injury to lung alveoli and respiratory failure with a significant reduction in the efficiency of the exchange of respiratory gases. Patients with ARDS are hospitalized for an extended period of time and suffer a long-term decrease in quality of life after recovery from the illness. Many ARDS survivors suffer long-term cognitive impairment and profound muscle atrophy. Innovative, beyond supportive, regenerative therapies using a cellular source are needed. Of the many cellular sources, UC-MSCs may be a special Stem Cell source of regenerative potential for repair of lung tissue damage in acute respiratory distress syndrome (ARDS).
Limitations Of Conventional Management
The current methods of management for acute respiratory distress syndrome (ARDS) are mainly supportive and include the use of mechanical ventilation, fluid management to reduce pulmonary edema, and the use of neuromuscular blocking agents to assist in lung rest. Even with these supportive care measures, the current therapies take time for the body to recover. These current therapies do not address the severe, life threatening hyperinflammation. It is also well known that prolonged mechanical ventilation will result in injury to lung tissue. These scenarios highlight the need for new Stem Cell therapies utilizing UC-MSCs that will modulate the injury and promote repair of lung tissue.
Biological Rationale and Immunomodulatory Mechanisms
The use of UC-MSCs offers the possibility of dealing with the injury of lung hyperinflammation in acute respiratory distress syndrome (ARDS) due to their strong immunomodulatory properties. This mesenchymal Stem Cell population is able to decrease the pulmonary cytokine storm. Acute Respiratory Distress Syndrome (ARDS) is characterized by immense neutrophil and macrophage migration to lung alveoli. TNF-α and IL-6 are two prominent pro-inflammatory mediators released in high quantities. UC-MSCs limit this response by releasing PGE2 and indoleamine 2,3-dioxygenase (IDO), which inhibit T-cell proliferation and promote regulatory T-cell differentiation, respectively. The effects of this Stem Cell treatment are rapidly restorative in nature due to their paracrine signaling.
Restoring The Alveolar Barrier
The therapeutic effects of T-cell suppression and regulatory T-cell promotion extend to repair and restoration of the alveolar-capillary barrier in acute respiratory distress syndrome (ARDS) as well. Regulatory T-cells assist in repair of tight junctions and the endothelial barrier of alveoli, which, when compromised, lead to a cascade of respiratory failure. UC-MSCs promote the proliferation of alveolar epithelial cells through the secretion of keratinocyte growth factor (KGF) and vascular endothelial growth factor (VEGF). The mesenchymal Stem Cell secretome contains microRNA within the extracellular vesicles, which transport the blocked apoptotic pathways and promote cellular survival within the injured tissues. With the maintenance of the lung structural components, the lung retains its architectural integrity even under maximum stress of inflammation.
Mitochondrial Transfer and Cellular Crosstalk
An additional aspect of the UC-MSCs mechanism of action as a Stem Cell therapy is the transfer of mitochondria. In severe pulmonary distress caused by acute respiratory distress syndrome (ARDS), alveolar macrophages are primarily affected by cell injury and subsequent loss of cellular respiration and energy. UC-MSCs donate mitochondria to injured immune and epithelial cells via tunneling nanotubes. This intercellular communication elevates and restores the cellular energy of the injured tissues. Substantial ATP production promotes the innate immune system’s clearing function without increasing inflammation. For this reason, the application of UC-MSCs alters the lung environment in acute respiratory distress syndrome (ARDS) from a destructive hyperinflammatory state to a constructive state of inflammation with a focus on resolution using Stem Cell mechanisms.
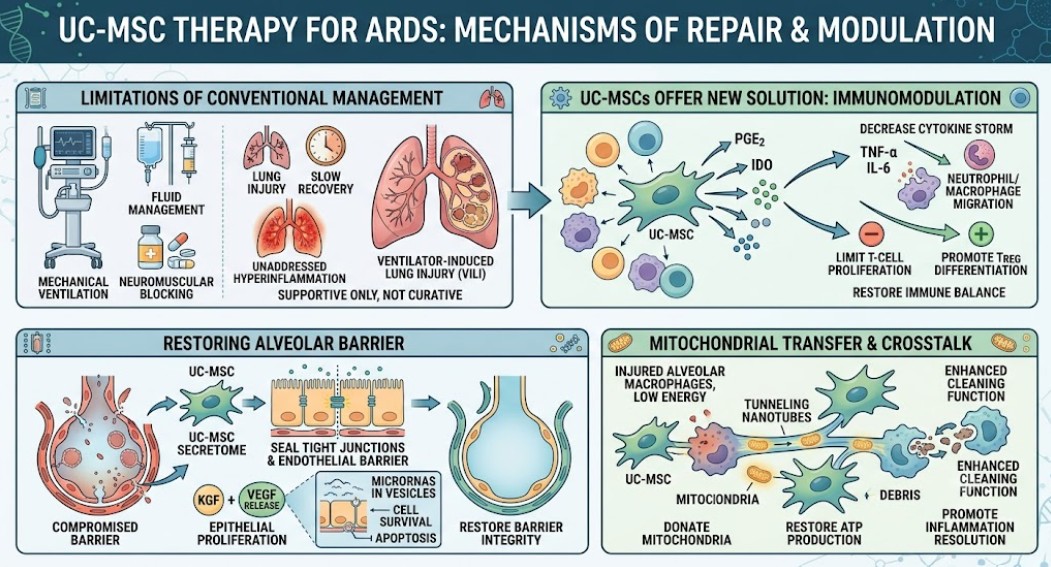
Figure 1: Mechanism of repair and modulation of UC-MSCs therapy for ARDS
Strategic Application in Thailand
The application of this advanced biological Stem Cell therapy within Thailand’s medical system is a good strategy. Thailand’s rapid development of biomedical services combined with world-class medical facilities is an advantage. Thailand’s specific geographic location has a tropical climate where there are periodic unusual outbreaks of infections that cause acute respiratory distress syndrome (ARDS). Severe respiratory viral infections and the complications of dengue fever are a constant burden to the Thai public health system. Developing local cultivation of UC-MSCs would give Thai medical professionals a rapid biological defense system to combat the severe respiratory distress syndrome when it occurs.
Also, Thailand has a legal system that is more open and flexible in developing and conducting Stem Cell clinical trials for regenerative medicine addressing acute respiratory distress syndrome (ARDS). The top universities in Bangkok lead research on advanced therapeutics, and sourcing UC-MSCs is very ethical from discarded umbilical cord tissue after childbirth. The collection of umbilical cord tissue is a non-invasive and painless medical procedure and is abundant in Thai maternity wards. Due to the low level of tissue immunogenicity, there is no need for HLA matching. This characteristic of universal donor makes it possible to use an “off-the-shelf” therapeutic product, which is ideal for emergency ICUs throughout Thailand.
Looking Ahead to the Future of Respiratory Care
Innovative Stem Cell research techniques utilizing UC-MSCs help Thailand lead the way in the treatment and management of respiratory care for acute respiratory distress syndrome (ARDS). With the global shift in healthcare towards precision regenerative medicine, the application of Stem Cell regenerative medicine protocols for severe lung injury in acute respiratory distress syndrome (ARDS) has the potential to dramatically improve patient outcomes. The unique and powerful immunomodulatory properties of UC-MSCs can change the approaches to the challenges of critical care pulmonary medicine and beyond. As this intervention goes beyond the limitations of traditional ventilation and begins to heal lung tissue at the molecular level, the potential for this technology to change the prognosis of patients with respiratory failure on a global scale is unprecedented.