

Ovarian aging is one of the most important biological limits in reproductive medicine. Unlike many organs that can renew cells continuously throughout life, the ovaries contain a finite follicle pool that gradually declines with time. As ovarian reserve decreases, the number of recruitable follicles becomes lower, hormone patterns may change, and response to fertility treatment may become less predictable. This decline can be part of natural reproductive aging, but it may also occur earlier than expected in women with diminished ovarian reserve, premature ovarian insufficiency, prior chemotherapy, ovarian surgery, endometriosis, autoimmune disease, genetic factors, or unexplained ovarian dysfunction.
The phrase “ovarian rejuvenation” has become popular in regenerative medicine marketing, but it should be used carefully. It can suggest that the ovary can be restored to a younger biological age, which is not proven. A more medically responsible term is ovarian function support or regenerative support for the ovarian microenvironment. This wording recognizes that emerging therapies may influence inflammation, oxidative stress, angiogenesis, stromal signaling, and follicular niche health, while avoiding the misleading idea that treatment can create unlimited new eggs or guarantee pregnancy.
Umbilical cord-derived mesenchymal stem cells, or UC-MSCs, are being studied because of their immunomodulatory, paracrine, angiogenic, anti-inflammatory, and tissue-supportive signaling properties. In ovarian research, interest focuses on whether these signals may help support granulosa cells, reduce oxidative injury, improve local vascular signaling, influence fibrosis, and create a more favorable environment for follicle development. Current reviews describe MSC-based strategies for ovarian aging and premature ovarian insufficiency as promising but still investigational, with many questions remaining about patient selection, delivery method, endpoints, and long-term outcomes.
Ovarian Reserve Is More Than a Number
Ovarian reserve refers to the quantity and, indirectly, the reproductive potential of remaining follicles. It is commonly assessed using anti-Müllerian hormone, or AMH, antral follicle count, or AFC, follicle-stimulating hormone, or FSH, estradiol, menstrual history, age, and ovarian response during stimulation. These tools help fertility specialists estimate how the ovaries may respond to treatment, especially IVF.
However, ovarian reserve tests do not tell the full story. ASRM notes that ovarian reserve declines with age, but ovarian reserve tests should not be treated as simple predictors of current natural fertility. They are more useful for predicting ovarian response to stimulation than guaranteeing whether a woman can or cannot conceive.
This distinction matters because regenerative medicine should not promise pregnancy based only on AMH or AFC changes. A patient may show improved ovarian markers without achieving pregnancy, while another may have low markers but still produce a usable oocyte. Fertility depends on many factors: age, egg quality, sperm quality, uterine health, tubal status, embryo genetics, endocrine balance, inflammation, lifestyle, and the IVF protocol when assisted reproduction is used.
Diminished Ovarian Reserve, POI, and Age-Related Decline Are Different
A high-quality article should separate three related but different clinical situations.
Diminished ovarian reserve usually means the ovary has fewer recruitable follicles than expected, often reflected by lower AMH, lower AFC, or higher FSH. Menstrual cycles may still be regular. Many women with diminished reserve are still ovulating, but may produce fewer eggs during stimulation.
Premature ovarian insufficiency, or POI, refers to loss of ovarian function before age 40, usually involving irregular or absent menstrual cycles with biochemical evidence of ovarian insufficiency. The updated ESHRE guideline defines POI as loss of ovarian function before age 40, indicated by irregular menstrual cycles together with biochemical confirmation.
Age-related ovarian decline is the natural reduction in follicle number and oocyte quality that occurs over time. This is not a disease, although it can significantly affect fertility planning.
UC-MSC stem cell therapy should not be discussed as if these three groups are the same. A 33-year-old with chemotherapy-related POI is biologically different from a 41-year-old with low AMH but regular cycles, or a 45-year-old with perimenopausal hormone changes. Regenerative planning must consider diagnosis, age, menstrual pattern, remaining follicle activity, IVF history, and overall reproductive goals.
The Follicular Microenvironment: The Real Target
The ovary is not only a storage site for eggs. It is a dynamic endocrine and reproductive organ made of follicles, granulosa cells, theca cells, stromal cells, blood vessels, immune cells, extracellular matrix, and signaling molecules. Follicle development depends on communication between the oocyte and surrounding granulosa cells. If the ovarian microenvironment becomes inflamed, poorly vascularized, fibrotic, or oxidatively stressed, follicle quality and responsiveness may decline.
This is where UC-MSC stem cell therapy becomes scientifically relevant. The proposed benefit is not that UC-MSC stem cell therapy directly become new eggs. The more defensible concept is that UC-MSC stem cell therapy may release biological signals that help regulate the ovarian niche. These signals may affect angiogenesis, apoptosis, inflammation, oxidative stress, extracellular matrix remodeling, and paracrine communication.
Recent mechanistic studies also discuss ferroptosis, mitochondrial stress, and extracellular vesicle-mediated signaling in ovarian insufficiency models, showing that ovarian dysfunction involves more than simple hormone deficiency.
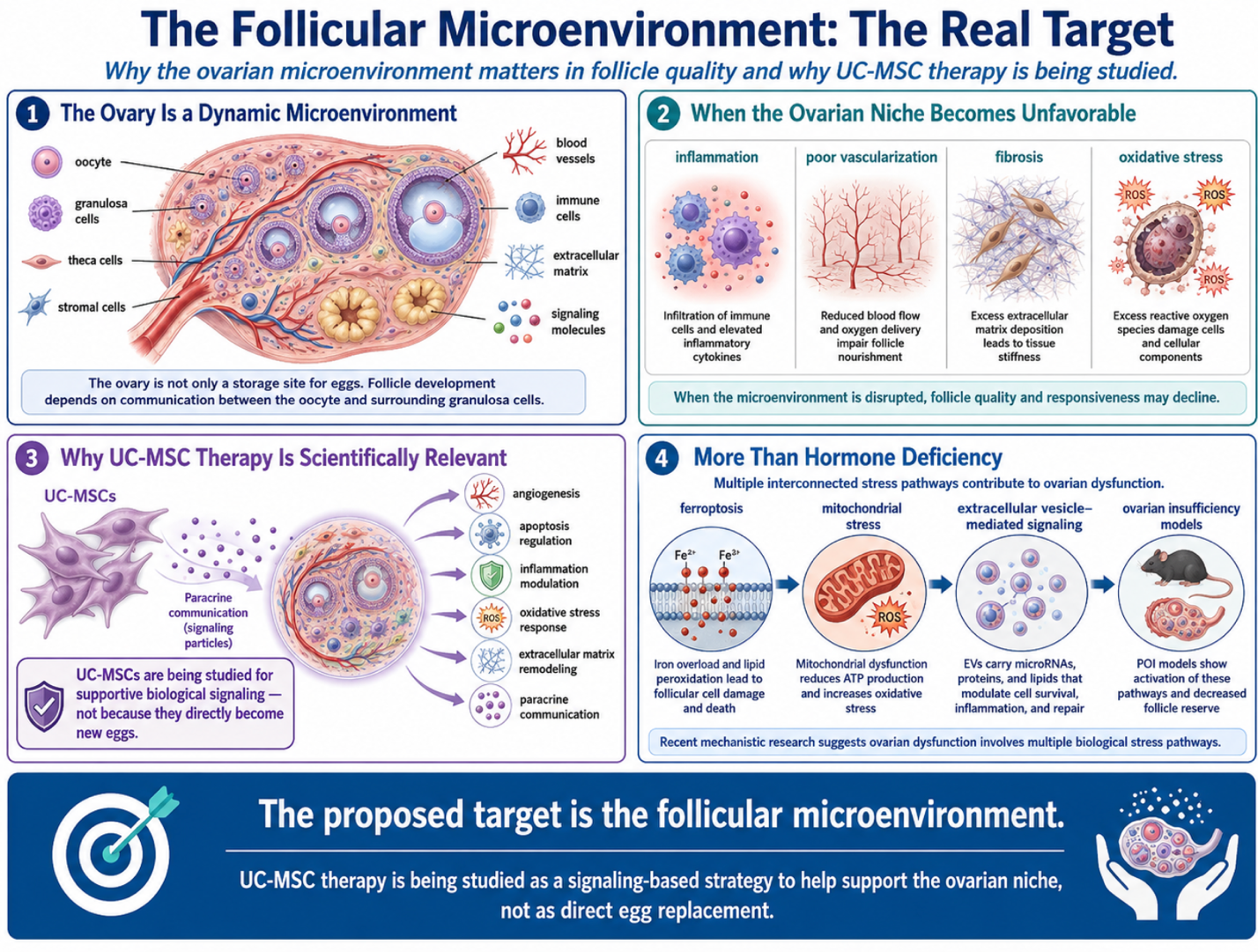
Figure 1: The Follicular Microenvironment as the Key Target in Ovarian Regenerative Therapy
What Are UC-MSC Stem Cell Therapy?
UC-MSC stem cell therapy are mesenchymal stem or stromal cells derived from Wharton’s jelly of the umbilical cord. This tissue is collected after healthy birth donation and processed under controlled laboratory conditions. UC-MSC stem cell therapy are studied because they are young, biologically active signaling cells with immunomodulatory and paracrine properties.
Their secreted products may include cytokines, growth factors, chemokines, microRNAs, extracellular vesicles, and regulatory proteins. In ovarian research, these signals are studied for possible effects on granulosa-cell survival, stromal repair, vascular signaling, anti-fibrotic pathways, oxidative stress reduction, and immune balance.
This means UC-MSC stem cell therapy should be described as supportive regenerative signaling, not direct egg replacement. The ovary’s follicle pool and oocyte quality remain major biological limits, especially with advancing age.
How UC-MSC Therapy May Support Ovarian Function
1. Granulosa-Cell and Follicular Support
Granulosa cells surround the oocyte and help regulate follicle growth, hormone production, and oocyte maturation. In ovarian aging or POI, granulosa cells may be affected by oxidative stress, apoptosis, mitochondrial dysfunction, and inflammatory signaling. UC-MSC-derived factors may support granulosa-cell survival pathways and reduce cellular stress in experimental models.
This may be relevant for patients who still have residual follicular activity. If no recruitable follicles remain, biological support may have limited reproductive effect.
2. Angiogenesis and Ovarian Blood Flow Signaling
Follicle development requires oxygen, nutrients, endocrine signaling, and waste removal. The ovarian stroma and follicular environment depend on microvascular function. UC-MSC stem cell therapy may release pro-angiogenic signals that support endothelial activity and local tissue perfusion. This does not mean treatment can guarantee improved blood flow or fertility, but angiogenic signaling is one reason MSC stem cell therapy are studied in ovarian insufficiency research.
3. Oxidative Stress Reduction
Oocytes and granulosa cells are sensitive to oxidative damage. Oxidative stress may impair mitochondrial function, DNA integrity, and follicle development. UC-MSC stem cell therapy and their extracellular vesicles are being studied for antioxidant and anti-apoptotic signaling. This is a plausible supportive mechanism, but it remains investigational in clinical fertility care.
4. Anti-Fibrotic and Stromal Support
Ovarian tissue can develop stromal fibrosis after inflammation, aging, surgery, chemotherapy, or chronic injury. Fibrosis can disrupt follicle signaling and tissue flexibility. UC-MSC stem cell therapy may influence extracellular matrix remodeling and anti-fibrotic pathways. This may be relevant in POI or poor ovarian response, but structural ovarian recovery is not guaranteed.
5. Extracellular Vesicle Communication
UC-MSC-derived extracellular vesicles carry proteins, lipids, and nucleic acids that may communicate with ovarian cells. In preclinical models, extracellular vesicles have been studied for effects on ovarian function, granulosa-cell pathways, and follicle survival. This area is promising, but clinical standardization is still developing.
Clinical Evidence: Promising but Not Settled
Clinical evidence for UC-MSC stem cell therapy in ovarian insufficiency is early. Reviews describe encouraging findings in POI and ovarian aging research, including changes in hormone profiles, follicle activity, and menstrual patterns in some studies. However, the field still faces major limitations: small study sizes, different cell sources, different routes of administration, variable doses, lack of standardized endpoints, and limited long-term follow-up.
A ClinicalTrials.gov pilot study on stem cells for premature ovarian failure investigated whether stem cell therapy could restore steroidogenesis, folliculogenesis, menstruation, and fertility, showing that this is still an area of formal investigation rather than established routine treatment. Another registered study is evaluating stem cell or stem cell-derived exosome therapy for gonadal failure, using hormonal changes and reproductive capacity as outcomes.
For patients, this means UC-MSC stem cell therapy should be presented as investigational supportive care, not a proven fertility treatment equal to IVF, donor eggs, or established reproductive medicine.
UC-MSC Therapy and IVF Planning
UC-MSC therapy may be discussed with women who have poor ovarian response, diminished ovarian reserve, or POI, especially when the goal is to support the ovarian environment before or alongside fertility planning. However, it should not replace consultation with a reproductive endocrinologist.
IVF planning may still require ovarian stimulation, ultrasound monitoring, hormone testing, egg retrieval, embryo development assessment, genetic counseling when appropriate, sperm evaluation, and uterine assessment. In some cases, donor eggs may remain the option with the highest chance of pregnancy, especially when ovarian reserve and oocyte quality are severely reduced.
A responsible article should explain that UC-MSC stem cell therapy may be considered as biological support, while IVF remains the established technology for fertilization, embryo culture, and embryo transfer.
Who May Be Considered?
Potential candidates may include selected women with diminished ovarian reserve, poor ovarian response to IVF, early POI with residual ovarian activity, chemotherapy-related ovarian injury after oncology clearance, or unexplained ovarian dysfunction after fertility specialist review.
Less suitable candidates may include women with active pelvic infection, untreated gynecologic cancer, severe endometriosis requiring surgical management, uncontrolled autoimmune disease, unstable endocrine disease, unexplained bleeding, severe uterine abnormalities, or no evidence of residual follicular activity. Age is also important, because egg quality declines with age even when ovarian markers change.
Evaluation should include age, menstrual history, AMH, AFC, FSH, estradiol, thyroid function, prolactin, reproductive history, IVF history, pelvic ultrasound, ovarian surgery history, chemotherapy or radiation history, autoimmune screening when relevant, partner sperm assessment, and fertility specialist opinion.
Safety, Cell Quality, and Route of Administration
For ovarian applications, safety is especially important because treatment may involve reproductive tissue. UC-MSC quality should include donor screening, infectious disease testing, sterility testing, endotoxin testing, viability assessment, identity markers, culture documentation, and physician-led handling.
Some protocols discuss intraovarian injection under ultrasound or laparoscopic guidance, while others discuss intravenous administration or cell-derived secretome approaches. Route selection should depend on medical indication, anatomy, safety review, and physician judgment. Local ovarian procedures require careful infection prevention, bleeding-risk assessment, and gynecologic expertise.
Regulatory language must also be cautious. The FDA warns that many regenerative medicine products marketed online have not been shown to be safe or effective and may expose patients to risk. It also notes that regenerative medicine products including stem cells and exosomes are regulated products, and misleading claims are common online. Regulations differ by country, but medical claims should remain transparent and evidence-aware.
Realistic Expectations
UC-MSC stem cell therapy should not be marketed as guaranteed ovarian rejuvenation, menopause reversal, or pregnancy restoration. More realistic goals may include supporting ovarian microenvironment health, reducing inflammatory stress, improving tissue signaling, supporting residual follicle activity, or preparing a more favorable biological setting for fertility treatment.
Progress should be tracked with objective measures such as menstrual pattern, AMH, AFC, FSH, estradiol, stimulation response, number of retrieved oocytes, embryo development, and pregnancy outcomes when IVF is used. These markers should be interpreted carefully because ovarian hormones can fluctuate and AMH changes do not automatically mean improved fertility.
For POI, standard care may still include hormone therapy for health protection when appropriate. ACOG states that hormone therapy in primary ovarian insufficiency can help reduce risks such as osteoporosis, cardiovascular disease, and urogenital atrophy and improve quality of life when no contraindications exist.
Conclusion
UC-MSC stem cell therapy for ovarian function should be discussed with scientific caution and reproductive medicine context. Ovarian decline involves follicle depletion, granulosa-cell stress, oxidative injury, vascular changes, stromal fibrosis, immune signaling, and endocrine disruption. UC-MSCs are being studied because they may influence several of these pathways through paracrine signaling, extracellular vesicles, immune modulation, angiogenesis, and anti-inflammatory effects.
However, “ovarian rejuvenation” should not be presented as a guaranteed reversal of aging or infertility. Current evidence remains early, and larger controlled trials are needed to define safety, efficacy, patient selection, route of administration, dosing, and reproductive outcomes.
For patients considering stem cell therapy for ovarian reserve or fertility support in Thailand, the safest pathway is fertility specialist review, clear diagnosis, high-quality UC-MSC preparation, realistic expectations, and continued reproductive care. Responsible regenerative fertility medicine should not promise pregnancy. It should support ovarian biology carefully, measure outcomes honestly, and work alongside established fertility planning.
FAQ
Can UC-MSC therapy reverse menopause?
No. UC-MSC therapy should not be described as a guaranteed menopause reversal treatment. It may be discussed as investigational ovarian function support in selected patients, especially when residual ovarian activity is present.
Can stem cell therapy guarantee pregnancy?
No. Pregnancy depends on ovarian reserve, egg quality, sperm quality, uterine health, embryo development, age, endocrine factors, and many other variables. UC-MSC therapy cannot guarantee pregnancy.
What is the difference between POI and diminished ovarian reserve?
POI is loss of ovarian function before age 40 with irregular menstrual cycles and biochemical confirmation. Diminished ovarian reserve usually means fewer recruitable follicles than expected, but menstrual cycles may still be regular.
Can UC-MSC therapy replace IVF?
No. UC-MSC therapy is not a replacement for IVF. It may be discussed as biological support before or alongside fertility treatment in selected patients.
What tests should be reviewed before treatment?
Important tests include AMH, AFC, FSH, estradiol, thyroid function, prolactin, pelvic ultrasound, menstrual history, reproductive history, IVF history, ovarian surgery history, and partner sperm evaluation.