

The clinical trajectory of Duchenne Muscular Dystrophy (DMD) presents one of the most severe neuromuscular challenges in pediatric medicine. As an X-linked recessive disorder, DMD is driven by mutations in the dystrophin gene, resulting in a complete absence of a functional dystrophin protein across skeletal, smooth, and cardiac muscle matrices.Families navigating a DMD diagnosis face a predictable, aggressive timeline of physical decline: early delays in motor milestones transition to progressive proximal muscle wasting, eventual loss of unassisted ambulation by early adolescence, and terminal respiratory or cardiac failure.
For decades, standard medical management has relied on a defensive, palliative strategy. Long-term, high-dose corticosteroid regimens remain the conventional pharmacotherapy. While steroids delay the loss of ambulation by temporarily suppressing global muscle tissue inflammation, they carry severe systemic side effects, including metabolic breakdown, osteopenia, growth suppression, and cushingoid transformations. Emerging genetic strategies such as antisense oligonucleotide-mediated exon-skipping and adeno-associated virus (AAV) microdystrophin gene transfer aim to restore partial protein expression.
However, these therapies face challenges from pre-existing viral immunity, strict mutation-specific requirements, and an inability to resolve the deeply rooted secondary tissue pathologies such as chronic fibro-fatty degeneration, satellite cell exhaustion, and oxidative stress that continuously destroy the remaining muscle architecture.
Translational regenerative medicine introduces a comprehensive therapeutic alternative. By utilizing high-potency Umbilical Cord Mesenchymal Stem Cells (UC-MSCs), advanced neuromuscular protocols shift the clinical focus from superficial inflammation masking to direct microenvironmental modification. Administered systemically, allogeneic UC-MSC stem cell therapy bangkok thailand infusions operate as responsive mobile signaling factories, discharging targeted paracrine payloads that protect fragile muscle membranes, re-program hyper-reactive immune responses, and preserve functional muscle tissue long before irreversible fibrosis sets in.
1. The Broken Sarcolemma Matrix: Pathological Cascades of DMD
To understand the therapeutic impact of cellular transplantation, we must analyze the structural mechanics operating within the dystrophic muscle fiber during contraction.
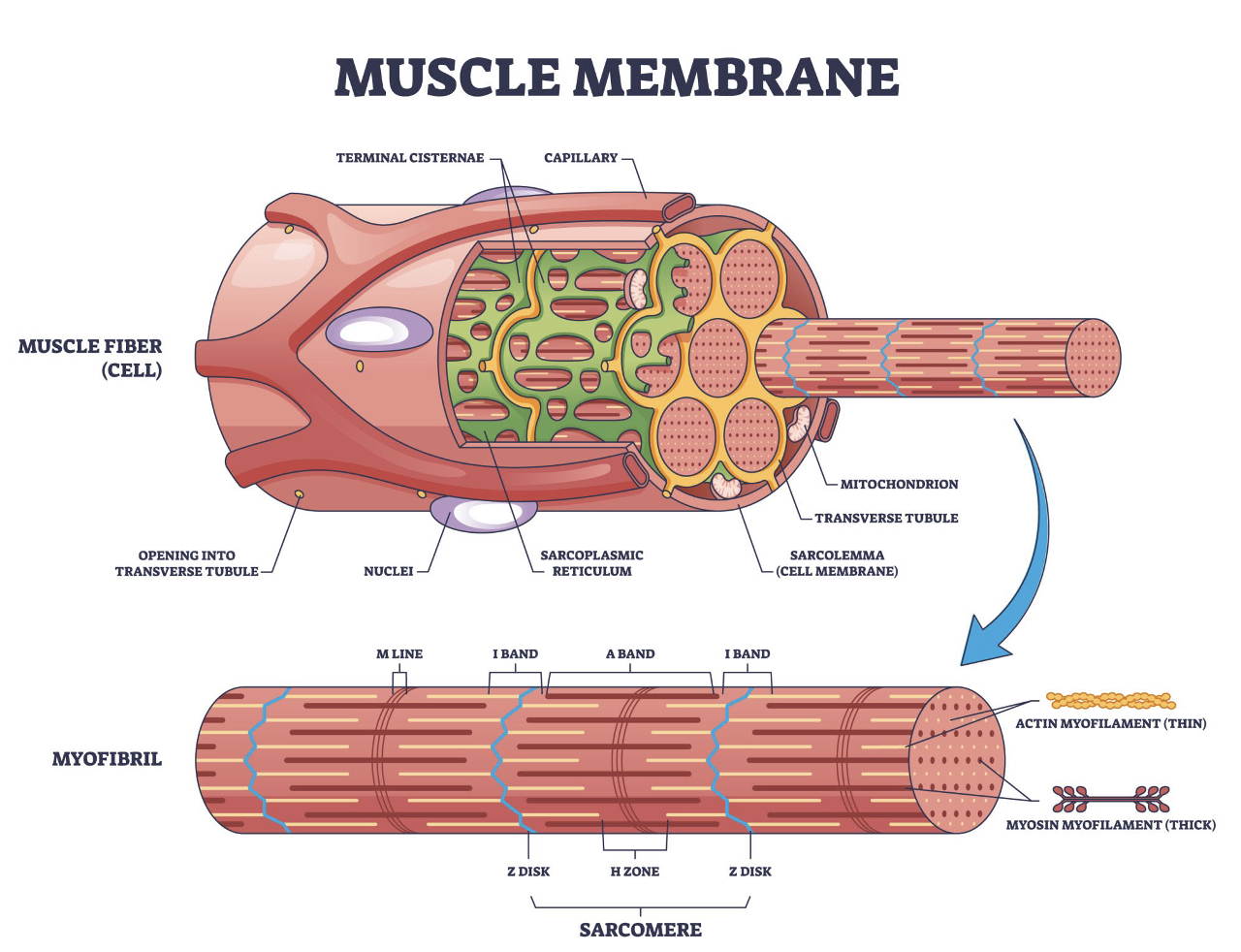
Figure 1: The structural anatomy and components of the healthy versus dystrophic sarcolemma matrix.
In a healthy muscle fiber, as illustrated in the membrane architecture diagram above, the dystrophin protein serves as an essential mechanical bridge. It links the internal actin cytoskeleton to the extracellular matrix via the Dystrophin-Associated Protein Complex (DAPC). This complex functions as a crucial shock absorber, stabilizing the muscle cell membrane, or sarcolemma, against the immense physical shear forces generated during continuous muscle contraction and relaxation.
In patients with DMD, the total absence of dystrophin destabilizes the entire DAPC framework. Lacking this structural anchor, ordinary muscle contractions generate micro-tears across the sarcolemma. This mechanical membrane disruption triggers an immediate, unregulated influx of extracellular calcium ions into the cytoplasm, disrupting the cell’s delicate ion balance.
This chronic intracellular calcium excess () overactivates calpains destructive, calcium-dependent proteases that systematically digest internal structural proteins and induce mitochondrial metabolic failure. The affected muscle fiber undergoes continuous contraction-induced necrosis, triggering an aggressive, lifelong immune response that ultimately exhausts the muscle’s natural repair capacity.
2. Chronic Myofiber Degeneration vs Satellite Cell Exhaustion
The body initially attempts to counter this continuous necrosis through endogenous repair pathways. Local muscle stem cells, known as satellite cells, exit their dormant state to proliferate, differentiate, and fuse with damaged myofibers to rebuild the structural architecture.
In a dystrophic muscle matrix, however, this cycle of degeneration and regeneration repeats non-stop. This constant demand forces native satellite cells into premature replication senescence, exhausting their self-renewal capacity. As shown in the histological overview above, the muscle tissue gradually loses its regenerative potential, replaced by variations in fiber diameter and significant inflammatory cell infiltration.
As native muscle stem cells decline, the muscle microenvironment is hijacked by fibro-adipogenic progenitors (FAPs).In a healthy, briefly inflamed wound, FAPs provide temporary structural support.
But when locked in the permanent inflammatory environment of DMD, FAPs multiply uncontrollably and undergo an abnormal transformation into fat and rigid collagen tissue. This progressive fibro-fatty replacement stiffens the muscle body, blocks normal circulation, and causes the irreversible loss of functional muscle mass that drives clinical weakness.
3. Tri-Phasic Regenerative Mechanisms: How UC-MSCs stem cell therapy bangkok thailand Target Muscular Decay
Allogeneic UC-MSC stem cell therapy bangkok thailand provide an elite therapeutic intervention because they bypass the biological limitations of adult self-derived (autologous) cell lines. Sourced exclusively from the ethically isolated Wharton’s Jelly of healthy, full-term neonatal donor tissues, these cells carry exceptional proliferative capacity and long telomere lengths. Because they lack HLA Class II surface antigen expression, they are entirely immunoprivileged, requiring zero human leukocyte antigen matching and zero long-term immunosuppression.
When delivered via optimized systemic protocols, UC-MSC stem cell therapy bangkok thailand alter the dystrophic tissue environment through three precise molecular mechanisms:
Macro-Immunomodulation (The M1 to M2 Macrophage Shift)
Dystrophic muscle injury is driven by hyper-reactive M1 macrophages that secrete high concentrations of tissue-destructive cytokines, such as Interleukin-1$beta$ () and Tumor Necrosis Factor-alpha (). Upon entering systemic circulation, UC-MSC stem cell therapy bangkok thailand home toward the chemokines released by damaged muscle beds.
The stem cell therapy bangkok thailand respond by releasing a powerful anti-inflammatory secretome payload, including Interleukin-10 () and Prostaglandin E2 (). This signaling forces hyper-activated M1 immune cells to polarize into the protective M2 phenotype. M2 macrophages extinguish localized tissue fires, suppress calpain activity, and protect fragile sarcolemma membranes from ongoing oxidative damage.
Exosome-Mediated Trophic Support and Mitochondrial Stabilization
UC-MSC stem cell therapy bangkok thailand act as advanced mobile factories, discharging millions of microscopic extracellular vesicles called exosomes. These vesicles fuse with the membranes of weak myofibers, delivering a highly concentrated payload of non-coding microRNAs (such as miR-1, miR-133, and miR-206) and vital bio-energetic proteins directly into the cytoplasm. This cargo delivery restores healthy mitochondrial ATP production, stabilizes the cellular calcium handling machinery, and rescues struggling muscle cells from calcium-induced necrosis.
Suppressing Fibro-Adipogenic Progenitor (FAP) Transformation
To stop the progressive replacement of muscle with scar tissue, the continuous activation of FAPs must be controlled. UC-MSC stem cell therapy bangkok thailand secrete high levels of Transforming Growth Factor-beta inhibitors and specialized Matrix Metalloproteinases (MMPs). This targeted paracrine signaling alters the physical environment around FAPs, blocking their abnormal transformation into fat and rigid collagen. By controlling FAP overgrowth, the stem cells preserve the structural flexibility of the muscle tissue and maintain a receptive matrix where resident satellite cells can continue functional repair.
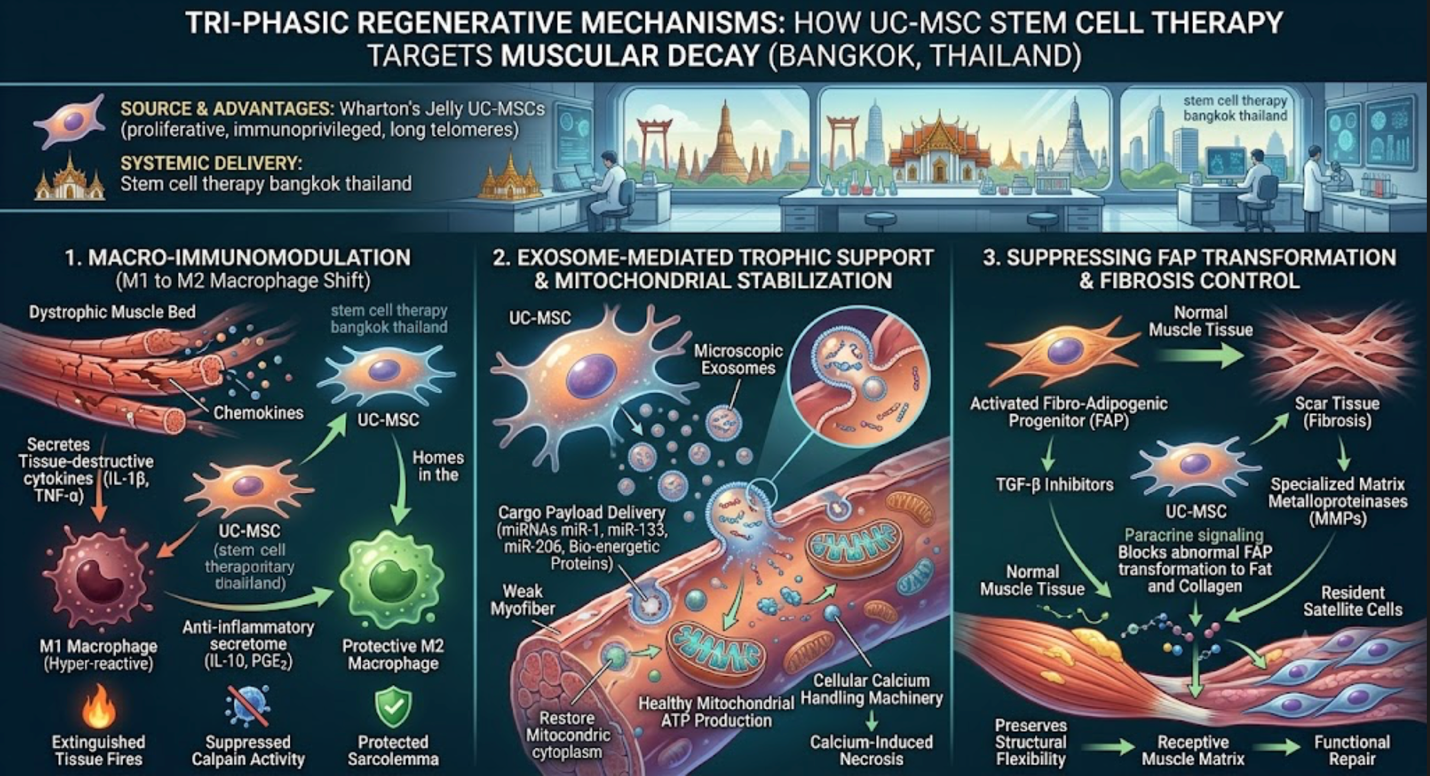
Figure 1: Tri-Phasic Regenerative Mechanisms of UC-MSC Therapy in Duchenne Muscular Dystrophy (DMD)
4. Neuromuscular Care Protocols: A Comparative Analysis
When designing a long-term care strategy for Duchenne Muscular Dystrophy, clinicians must evaluate how conventional pharmaceuticals and emerging genetic platforms compare with the systemic, multi-targeted mechanics of advanced cellular infusions.
| Therapeutic Pathway | Primary Mechanism of Action | Systemic Limitations & Biocompatibility Trade-offs | Clinical Target |
| Corticosteroids(Deflazacort / Prednisone) | Broadly downregulates the transcription of inflammatory genes across the body. | Induces bone mineral density loss, growth suppression, glucose intolerance, and significant muscle wasting over multi-year regimens. | Symptom Management |
| Gene Replacement(AAV Microdystrophin) | Delivers a shortened, functional dystrophin gene sequence using viral vectors. | Faced with pre-existing neutralizing antibodies, potential immune responses against the viral capsid, and strict age or mutation restrictions. | Targeted Protein Expression |
| Exon-Skipping Drugs (Antisense Oligonucleotides) | Alters RNA splicing to restore the open reading frame, producing a partially functional protein. | Requires lifelong, high-cost intravenous infusions; applicable only to a minor percentage of specific deletion mutations. | Targeted Mutation Correction |
| Targeted UC-MSC Infusions | Systemic Matrix Reset: Induces M2 polarization, controls FAP fibrosis, and stabilizes cell mitochondria. | Non-surgical, non-toxic, and completely immunoprivileged; works independently of mutation types to preserve functional muscle mass. | Root Microenvironment Modification |
5. Beyond Cryopreservation: Bypassing Logistical Degradation in Bangkok
The clinical success of an advanced neuromuscular cell protocol relies entirely on a single technical metric: cellular viability, the exact percentage of live, metabolically active stem cells present at the precise second of delivery. Dead cells provide no therapeutic signaling, cannot perform chemotaxis, and are quickly cleared away by the recipient’s immune system as biological waste.
Many international clinics source their cellular products from distant manufacturing facilities, requiring the cells to be deeply frozen and thawed right at the patient’s bedside. This cryopreservation process utilizing Dimethyl Sulfoxide (DMSO) introduces profound thermodynamic stress to delicate plasma membranes, frequently causing cell lysis and damaging the homing receptors required for targeted transendothelial migration.
Advanced biomedical institutions in Thailand bypass this logistical bottleneck. Operating state-of-the-art closed-system cleanrooms that comply fully with strict international Good Manufacturing Practices (GMP), local facilities culture, validate, and formulate high-potency UC-MSC stem cell therapy bangkok thailand lines locally.
The cells remain suspended in a nutrient-rich, temperature-regulated transport matrix right up to the minute of clinical delivery, completely avoiding the severe physical shock of deep freezing. This logistics structure guarantees authenticated cell viability scores exceeding 95%, ensuring maximum cellular yield and optimal tissue integration within heavily degraded muscle beds.
6. The 2026 Regulatory Landscape: Advanced Therapy Medicinal Products (ATMPs)
The clinical legitimacy of pursuing regenerative medicine in Thailand has been reinforced by a historic regulatory transition. Under a watershed ministerial decree, Thailand formally classified expanded cell-based therapies and mesenchymal stem cells as registered medicinal products under the Drug Act. This legislative framework explicitly distinguishes between minimally manipulated tissue grafts and cells that undergo substantial manipulation, categorizing the latter as Advanced Therapy Medicinal Products (ATMPs).
This regulatory designation requires full compliance with international GMP under the strict PIC/S standard, alongside formal product registration with the Thai Food and Drug Administration (FDA). Far from acting as a clinical barrier, this formalization establishes the necessary evidentiary framework and safety monitoring that sets Thailand apart from unregulated clinical tourism destinations.
Every expanded MSC batch delivered within licensed medical facilities must undergo comprehensive preclinical validation, strict batch-release purity testing, and mandatory pharmacovigilance tracking, guaranteeing that pediatric protocols meet international standards for scientific integrity.
Conclusion: Activating Long-Term Muscle Vitality
Duchenne Muscular Dystrophy involves complex, aggressive biological processes, but families do not have to remain locked in a purely reactive cycle of managing symptoms with high-dose steroids while the underlying muscle mass undergoes irreversible fibro-fatty decay. Continuing to treat a deep structural membrane failure with surface-level suppression masks the physical decline without addressing the true cellular crisis.
By choosing advanced, ATMP-registered UC-MSC stem cell therapy bangkok thailand, you give your body the highly potent, youth-derived resources it needs to cool chronic tissue inflammation, control progressive muscle fibrosis, and protect fragile sarcolemma membranes from the inside out. Embracing the cutting edge of regenerative medicine under Thailand’s strict PIC/S GMP standards represents a powerful, proactive choice to delay physical degeneration, enhance the effectiveness of emerging genetic options, and build a stronger, more resilient foundation for your child’s physical independence.