

The management of complex rotator cuff tears, chronic subacromial bursitis, and glenohumeral arthropathy presents an intricate structural challenge within contemporary orthopedics. The shoulder joint complex features the greatest range of motion of any diarthrodial joint in the human body, relying on a delicate balance between negative intra-articular pressure, passive labral anchors, and active muscular compression.
Because of this intense biomechanical demand, structural assets like the supraspinatus tendon are highly susceptible to acute macrotrauma and chronic, age-related mechanical failure. When a patient experiences dynamic shoulder degradation, they face a progressive loss of physical capability characterized by severe night pain, mechanical catching, shoulder instability, and an inability to execute overhead abduction.
Conventional orthopedic strategies for managing shoulder lesions operate under a distinctly reactive, palliative framework. Standard clinical protocols focus on managing surface-level symptoms: oral non-steroidal anti-inflammatory drugs (NSAIDs), temporary immobilization slinging, and repetitive subacromial or intra-articular corticosteroid injections. While these foundational interventions provide temporary pain relief, they do not correct the underlying microenvironmental failures driving the decay.
Long-term dependency on anti-inflammatory medications carries well-documented risks of gastrointestinal and cardiorenal toxicity. Concurrently, repeated corticosteroid injections accelerate native cartilage and tendon breakdown by suppressing resident cell metabolism and driving local tenocytes or chondrocytes into premature programmed cell death (apoptosis). Once mechanical erosion results in complete muscle detachment or severe bone-on-bone friction, surgical options are exhaustively restricted to invasive reconstructive procedures like arthroscopic rotator cuff repair, subacromial decompression, or total reverse shoulder arthroplasty.
Translational medicine introduces a proactive alternative to this paradigm through Regenerative Musculoskeletal Care. By utilizing high-potency, youth-derived neonatal Umbilical Cord Mesenchymal Stem Cells (UC-MSCs), advanced protocols of stem cell therapy bangkok thailand shift the treatment framework from superficial symptom suppression to direct microenvironmental modification.
Administered via precise target-assisted delivery vectors, these immunoprivileged allogeneic cell lines act as responsive mobile signaling factories suppressing chronic subacromial lining inflammation, rescuing weak resident cells from oxidative collapse, and actively driving the synthesis of an organized extracellular matrix (ECM) to achieve true joint and structural tissue preservation.
1. The Biomechanical Crisis: Microenvironmental Decay in Shoulder Pathologies
To understand why traditional treatments fall short and how advanced stem cell therapy bangkok thailand alters clinical outcomes, the pathological lens must examine the precise microenvironmental variations occurring within degraded shoulder tissues. The glenohumeral joint and surrounding rotator cuff tendons rely on a delicate homeostatic balance managed by specialized cell populations residing within dense extracellular matrices.
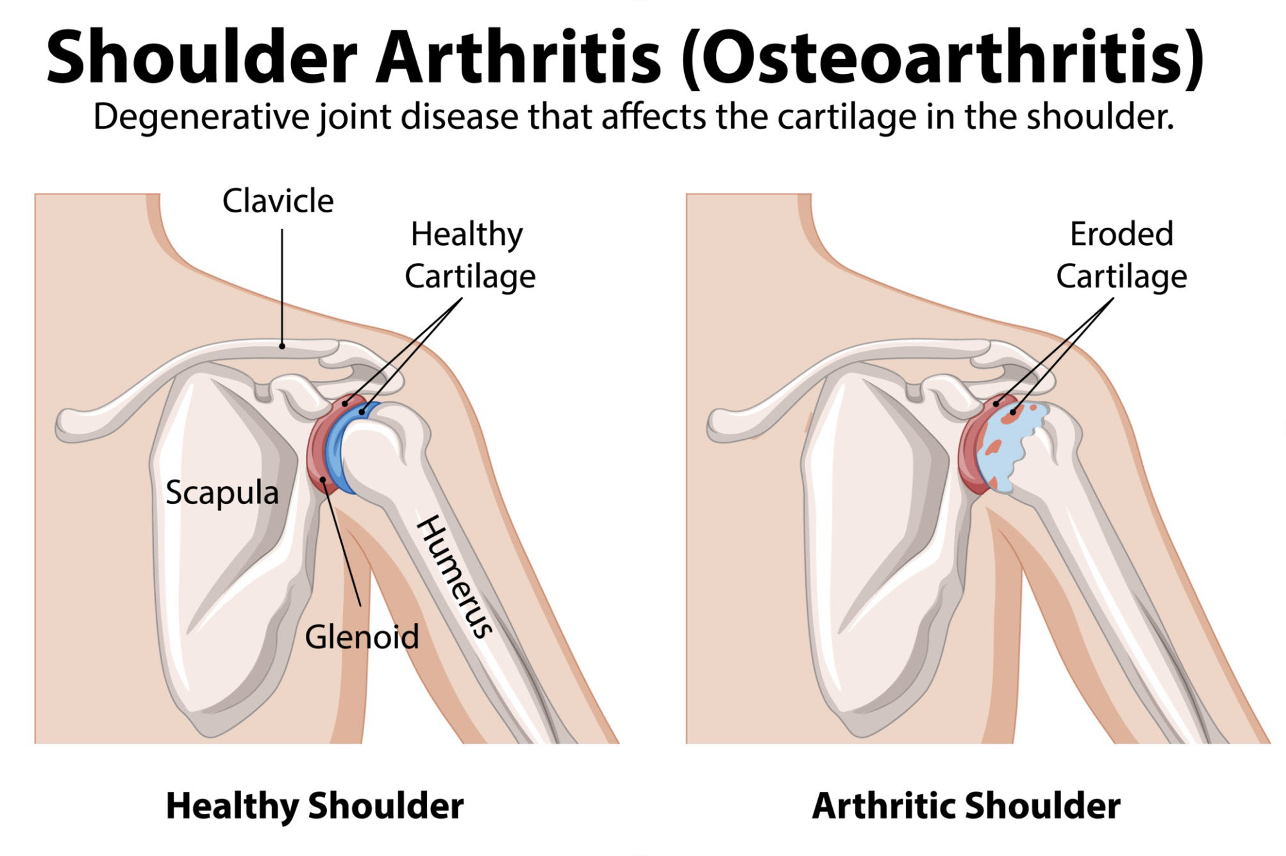
The structural pathomechanisms of cartilage matrix erosion in shoulder arthritis. Source: colematt / Getty Images
As shown in the anatomical comparison above, a healthy shoulder joint utilizes clean, uncompromised articular surfaces to distribute loading forces evenly across the glenoid cavity. When a shoulder structure experiences mechanical trauma, poor circulation within the “critical zone” of Codman, or chronic subacromial impingement, this baseline equilibrium fractures completely. The initial breakdown of normal matrix structures triggers a localized, destructive auto-inflammatory cascade.
Mechanical shearing forces damage the superficial cartilage or tendon fibers, releasing microscopic matrix debris into the synovial fluid. The resident immune cells mistake this tissue waste for an active pathological threat, inducing a state of chronic local tissue inflammation. Hyper-activated white blood cells and nearby synoviocytes flood the joint cavity with a destructive wave of pro-inflammatory cytokines, including Interleukin-1β (IL-1$beta$), Interleukin-6 (IL-6), and Tumor Necrosis Factor-alpha (TNF-).
This chronic chemical bath induces the upregulation of destructive catabolic enzymes called Matrix Metalloproteinases (MMPs). These enzymes aggressively digest Type I and Type II collagen strands, stripping away the proteoglycan framework. Starved of vital matrix support and exposed to persistent oxidative stress, local tenocytes undergo rapid apoptosis, permanently compromising the body’s natural capacity for self-repair and establishing the progressive tissue erosion that defines advanced cases requiring Regenerative Musculoskeletal Care.
2. The Structural Interface: Mapping the Tendon-to-Bone Enthesis Matrix
The primary biological roadblock preventing independent shoulder recovery in long-standing rotator cuff pathologies is the degradation of the highly specialized structural boundary known as the enthesis matrix. Rotator cuff tendons do not insert into bone as simple fibrous ropes; instead, they transition through a precisely organized, four-zone interface engineered to distribute mechanical shear stresses safely.
The structural zones and cellular components of the healthy tendon-to-bone insertion. Source: Frontiers
When you analyze the structural transition of a healthy enthesis interface in the illustration above, notice the precise four-zone matrix organization:
Pure Tendon Zone: Composed mainly of highly aligned, parallel Type I collagen fibers interspersed with functional proteoglycans and resting tenocytes.
Unmineralized Fibrocartilage Zone: A flexible transition matrix where the tissue layout shifts, displaying a high density of round chondrocyte cells embedded within a complex web of Type II and Type X collagen strands.
Mineralized Fibrocartilage Zone: A rigid structural barrier characterized by gradual collagen mineralization and hypertrophic chondrocytes, designed to lock the insertion securely.
Bone Zone: The final hard anchor matrix where the mineralized fibers integrate directly into the subchondral bone layers.
In chronic rotator cuff tears and advanced tendinopathies, this precise four-zone interface is completely dismantled and replaced by disorganized, biomechanically weak scar tissue. When fibro-adipogenic progenitors (FAPs) hijack the injury site, they deposit loose, chaotic configurations of Type III collagen instead of parallel Type I fibers.
This unorganized scar tissue lacks the necessary elasticity and tensile strength to handle rotational loading forces, leading to a high rate of structural failure and re-tearing following conventional surgical suturing. By implementing stem cell therapy bangkok thailand, medical protocols seek to deliver specific paracrine instructions that systematically suppress FAP overgrowth, helping the body re-establish an organized fibrocartilage transition zone during tissue remodeling.
3. Molecular Mechanisms of Action: How UC-MSC stem cell therapy bangkok thailand Rebuild the Musculoskeletal Niche
Allogeneic Umbilical Cord Mesenchymal Stem Cells introduce a highly advanced biological intervention for Regenerative Musculoskeletal Care because they bypass the biological limitations, environmental mutations, and cellular fatigue that compromise adult self-derived (autologous) bone marrow or fat extractions. Sourced exclusively from the ethically isolated Wharton’s Jelly of healthy, full-term neonatal donor tissues, these cells carry exceptional proliferative capacity and extended telomere lengths. Because they lack HLA Class II surface antigen expression, they are entirely immunoprivileged, requiring zero human leukocyte antigen matching and zero long-term immunosuppression.
When delivered through optimized clinical protocols of stem cell therapy bangkok thailand, UC-MSC stem cell therapy bangkok thailand alter the degraded microenvironment of the shoulder joint through three precise molecular mechanisms:
Macro-Immunomodulation and Synovial Flammability Reduction
Once injected into the inflamed subaromial bursa or glenohumeral capsule, UC-MSC stem cell therapy bangkok thailand sense the high concentration of pro-inflammatory cytokines through specific surface receptors. The stem cells respond by releasing a powerful anti-inflammatory secretome payload, including Interleukin-10 (IL-10), Prostaglandin E2 (PGE2), and Transforming Growth Factor-beta (TGF-). This localized release neutralizes circulating IL-1 and TNF-, forcing destructive M1 macrophages within the synovial lining to polarize into a calming, protective M2 repair phenotype. This structural switch turns off the local tissue fire, stabilizing the environment so that matrix-building repair processes can survive.
Exosome-Mediated Tenocyte Rescue and Mitochondrial Stabilization
UC-MSC stem cell therapy bangkok thailand function as advanced mobile factories, discharging millions of microscopic, membrane-bound extracellular vesicles called exosomes into the tissue space. These vesicles traverse dense tendinous boundaries to fuse with the plasma membranes of weak, struggling native tenocytes and chondrocytes, delivering a highly concentrated payload of non-coding microRNAs (such as miR-29 and miR-140) directly into the cytoplasm. This cargo delivery restores healthy mitochondrial ATP energy production, downregulates pro-apoptotic Bax genes, and rescues surviving structural cells from premature death, preventing further tearing of the tendon body.
Neo-Angiogenesis and Extracellular Matrix Synthesis
To close physical erosion defects on tendinous and articular surfaces, the extracellular matrix must be actively rebuilt. Because the rotator cuff’s insertion zone features a naturally poor blood supply (the critical zone of Codman), injuries are frequently held back by structural ischemia. UC-MSCs actively resolve this restriction by secreting high concentrations of Vascular Endothelial Growth Factor (VEGF) and basic Fibroblast Growth Factor (bFGF), which drive micro-capillary sprouting to restore local oxygen delivery.
Simultaneously, the stem cells secrete Transforming Growth Factor-beta 3 (TGF-), which acts like a direct biological instruction that commands local cells to synthesize high-quality Type I collagen and aggrecan, rebuilding an organized, aligned structural framework across the enthesis interface.
5.Real-World Expectations: Defining Objective Orthopedic Progress
When discussing advanced cellular therapies for shoulder chronic injuries, maintaining absolute honesty, transparency, and a grounded perspective is essential. Stem cell therapy is not a magical overnight cure that will instantly eliminate high-grade mechanical gaps or wipe away years of physical damage in a single day. Instead, it serves as a powerful biological accelerant that works hand-in-hand with clinical management to slow the progression of the disease and create conditions where structural tissue can gradually recover.
Patients who respond well to advanced orthopedic protocols typically report gradual, steady health improvements over a window of two to six months:
Mitigation of Night Pain: A measurable reduction in the frequency and intensity of throbbing or deep architectural pain, driven by the down-regulation of inflammatory cytokines within the subacromial bursa cavity.
Recovery of Range of Motion: A progressive return of pain-free passive and active shoulder abduction, flexion, and internal rotation, supporting daily functional mobility.
Reversal of Mechanical Catching: A visible smoothing of joint mechanics, reducing painful catching or crepitus during overhead lifting tasks.
Stabilized Structural Integrity: High-resolution follow-up ultrasounds or MRIs frequently reveal a visible stabilization or progressive remodeling of the tendon-to-bone enthesis boundary.
Conclusion: Reclaiming Control of Your Physical Flexibility
Degenerative shoulder arthritis, chronic tendinopathy, and rotator cuff matrix loss involve progressive biological processes, but patients do not have to remain locked in a purely reactive cycle of managing pain with temporary steroid blocks while the underlying structural tissue undergoes permanent decay. Continuing to treat a deep mechanical and cellular matrix failure with simple surface-level chemical suppression masks the physical decline without addressing the true structural crisis.
By choosing advanced, ATMP-registered stem cell therapy bangkok thailand, you give your body the highly potent, youth-derived resources it needs to cool chronic synovitis, protect surviving tenocytes or chondrocytes, and rebuild a resilient proteoglycan scaffold from the inside out. Embracing the cutting edge of regenerative medicine under Thailand’s strict PIC/S GMP standards represents a powerful, proactive choice to avoid the constraints of joint-fusing or artificial reconstructive surgeries, preserve your natural structural flexibility, and reclaim a vibrant foundation of long-term health and physical independence through comprehensive Regenerative Musculoskeletal Care.