

ASD, which is short for autism spectrum disorder, represents a vast and generalized neurodevelopmental disorder that can have an impact on communication, behavior, sensory processing, focus attention sweet digestive function participation in learning and daily adaptive skills. Since the biological and clinical presentation of autism varies from person to individual, many households are searching for broader assisting therapies, which include UC-MSC Thailand, stem cell therapy for autism, and regenerative medicine for autism assisting approaches.
Umbilical cord-derived mesenchymal stem/stromal cells (UC-MSCs) have attracted much attention due to the potential function of immune regulation, inflammatory modulation, paracrine signaling and tissue supportive communication in regenerative medicine. Despite the advantages UC-MSCs, it is best to characterize their use as an investigational supportive option as opposed to a defined curative or replacement for standard developmental therapies. Biology may hold promise based on recent data, but larger controlled trials, standardised protocols, long-term safety monitoring and clearer selection criteria are still needed.
UC-MSC Thailand, stem cell for autism, practical guide to autism keyword blog Tags: gene vault gao regenerative medicine research needs in the pathway stay up – These expertise are all excellent practices that could have a serious impact on helping an individual with disability and spur local economies.
Autism families seek UC-MSC-Based support
Autism spectrum disorder is not a single symptom in one domain. It can relate to aspects of social interaction, communication style, repetitive behaviors, sensory sensitivity and regulation, emotional regulation and management, wake/ sleep cycles, gastrointestinal comfort and functional independence. Care is typically individualized and multidisciplinary since each child has a distinct profile of strengths and challenges.
This complexity is also an important reason that families will look for UC-MSC Thailand and stem cell therapy for autism. For many parents, there may not be only a single treatment they are interested in exploring, but rather supportive treatments that might address biological factors which may include immune activity, inflammation, oxidative stress, gut-brain communication. and the neurodevelopmental microenvironment balance.
Autism regenerative approaches have yet to be established and these therapies should not be advertised as effective treatment, logical (in that order), or alternate modalities for occupational therapy, speech-language pathologic intervention, behavioral teacher special education services professions pediatric neurology.
Biological rationale: why are you studying autism using UC-MSCs?
UC-MSCs are mesenchymal stem/stromal cells obtained from umbilical cord tissue. They are sought after in regenerative medicine as they can secrete biologically active molecules such as growth factors, cytokines, extracellular vesicles and other signaling constituents.
They are primarily supposed to have a role in cell signalling, so not directly replacing tissue. In other words, UC-MSCs are not studied since they just become new brain cells. Rather, the scientific question is how much their secreted factors might tilt the balance of immunity or drive inflammatory signaling, vascular support, tissue repair communication and/or surrounding cell milieu.
These properties are relevant to autism research because several studies address the potential biologic association between ASD and immune dysregulation, neuroinflammation, oxidative stress, gastrointestinal dysbiosis, and abnormal gut-brain interactions. Not all of these mechanisms are applicable to each child, but they may account in part for the recent surge of interest in UC-MSCs as a potential regenerative therapeutic strategy for autism.
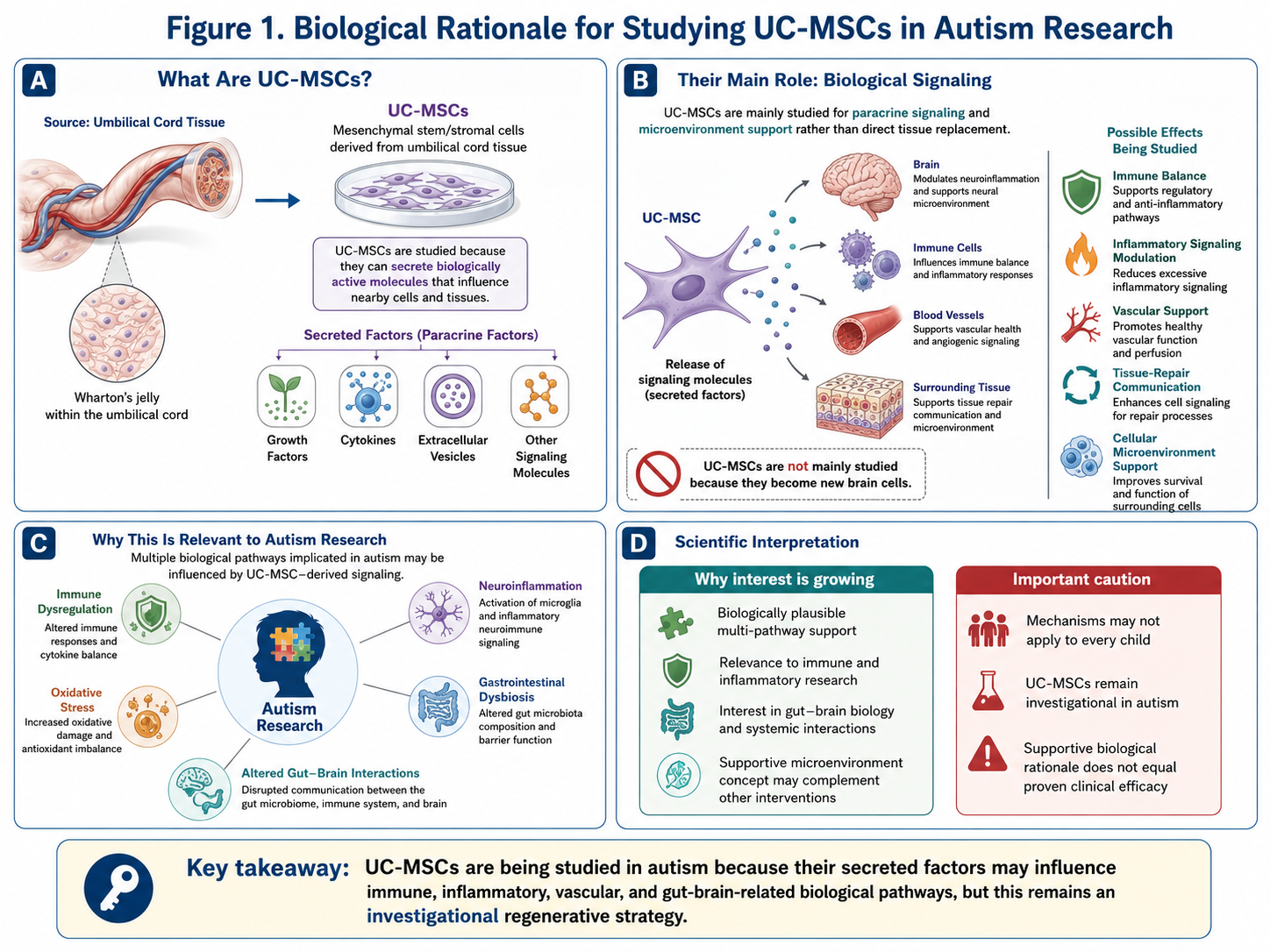
Figure A: Biological Rationale for Studying UC-MSCs in Autism Research
Potential Mechanisms through which UC-MSCs may provide Support in Autism
3.1 Immune Regulation
Some children with autism may have signs of immune imbalance or inflammatory activity. UC-MSCs have been examined for their capacity to modulate immune-cell activity and to enable a more even-handed immune response. This is part of the reason why they are talked about in some autism support programs.
3.2 Anti-Inflammatory Signaling
UC-MSCs may release soluble factors that modulate inflammatory responses. This possible effect is still being studied and should not be construed as an established clinical endpoint.
3.3 Gut-Brain Axis Communication
This review aims to encompass one of the most intriguing fields of autism studies, being part of gut-brain axis. Gastrointestinal and other associated disorders Many children often show symptoms of digestive disturbance due to ASD such as food sensitivity, alter in bowel alteration or gut-associated behavioral change. We summarize some recent findings on mammalian UC-MSC-related paracrine signaling as well as extracellular vesicles (EVs), and their possible roles in regulating gut-immune-brain communication.
3.4 Oxidative Stress Modulation
In certain neurodevelopmental and inflammatory conditions, cellular dysfunction may be attributable to oxidative stress. The potential of UC-MSCs to support cellular stress homeostasis also merits evaluation and the effects mediated through secreted bioactive factors.
3.5 Neurodevelopmental Microenvironment Support
One possible explanation is that UC-MSCs provide support for the biological milieu in and surrounding neurodevelopmental pathways. This might include communication via trophic signaling, immune regulation, inflammatory balance and vascular-supportive communication. This is not to intend neural replacement, but rather to outline an additional biological support system that may serve and underpin the framework.
Aggregate Evidence: What the Research Shows You
Stem cell therapy for autism is still in its early stages, with limited clinical evidence. Few studies have reported results of umbilical cord-derived cell products in children with ASD during their early phases and observed feasibility or promising observations. Nonetheless, these results need to be interpreted with caution because most studies were performed on small series, cell sources, doses and routes of administration varied and long-term follow-up is usually limited.
While systematic reviews and review papers have typically noted the scientifically interesting potential for this field to be translated into a standard autism therapy, they have also often cautioned that it may not yet be sufficiently mature for such definitions to occur when considering UC-MSCs in a general sense. Studies of safety, beneficial dosage, treatment frequency and route of admission, suitability for specific form of patients and measurable developmental markers require a randomized controlled trial.
This is why UC-MSCs should be viewed as an investigational supportive strategy rather than a validated treatment.
Why UC-MSCs Might Be Available in Certain Autism Classes
Given their biologically plausible multiple models of action, UC-MSCs should be considered for selected physician supervised autism treatment programs.
The main reasons include:
Potential immune-modulating activity
Possible anti-inflammatory signaling
Interest in gut-immune-brain communication
Possible oxidative stress support
Neurodevelopmental microenvironment support
Compatibility with multidisciplinary developmental care
But it should be noted that just because they offer UC-MSCs does not mean the therapy works for autism. Hence, some medical teams might apply UC-MSCs within a broader supportive framework but be careful in their communication regarding variable outcomes and developing evidence.
Monitoring of Possible Areas After UC-MSC Support
In discussing potential benefits, keep the language tentative. Clinicians might talk about areas to watch and monitor, rather than make guarantees of improvement.
These may include:
Attention and engagement
Eye contact and social awareness
Sleep quality
Emotional regulation
Sensory tolerance
Communication attempts
Repetitive behavior patterns
Digestive comfort
Participation in learning activities
Daily adaptive function
Children can respond very differently, Other variables that may impact observed outcomes include age, baseline developmental status, autistic severity or subtype of autism (e.g., inflammatory profile), sleep parameters, gastrointestinal health and immune status; nutrition; intensity of therapy delivery including intensity and duration of application.
Patient Selection and Safety Considerations
The right way for a UC-MSC Thailand autism support program should begin with an in-depth medical and developmental evaluation. This will help with assessments, safety and monitoring progress.
However, these more critical areas may include:
Confirmed autism diagnosis
Developmental and behavioral history
Speech and communication level
Sensory processing profile
Sleep pattern
Gastrointestinal symptoms
Seizure history
Allergy or immune background
Current medications and supplements
Previous therapies and response
Nutritional status
Pediatric or neurological review
UC-MSC–based support should be linked with established developmental care (occupation/speech therapy, behavioral support, educational planning, nutrition, sleep).
Conclusion
Since UC-MSCs offered a unique exploration into regenerative strategies for autism, in terms of immune regulation, inflammatory equilibrium, paracrine signaling pathways, gut-brain axis communication potential, oxidant injury support and glycoprotein modulation of the neurodevelopmental microenvironment, we also address this particular treatment branch below. As a result, UC-MSC Thailand has become increasingly researched by families interested in finding therapeutic options in autism care.
Nevertheless, the most reasonable conclusion is that UC-MSCs are still investigational for autism. Findings so far are promising, but larger clinical trials, standardized dosing techniques, long-term safety studies, and better models to select patients need to be performed.
Accordingly, UC-MSCs need to be presented as an adjunctive treatment option under the supervision of a physician and not as a cure or an alternative to established developmental therapies. The least specious model of autism treatment is probably a cautious scientific approach with modest expectations, research-established conditions for successful cell procurement; multidisciplinary long-term therapies and well-designed follow-up.