

Crohn’s disease is a chronic, relapsing form of inflammatory bowel disease (IBD) that can affect any part of the digestive tract, from the mouth to the anus. Unlike ulcerative colitis, which is usually limited to the colon and inner mucosal lining, Crohn’s disease can involve the deeper layers of the bowel wall. This transmural inflammation helps explain why the condition may cause chronic diarrhea, abdominal pain, fatigue, malnutrition, strictures, abscesses, and perianal fistulas.
For many patients, Crohn’s disease is not only about controlling a flare. It is about living with a long-term immune-mediated condition that may return in cycles and gradually affect nutrition, daily routine, work, school, travel, and quality of life. Standard care has improved significantly with corticosteroids, immunomodulators, biologic therapy, small molecules, nutritional support, endoscopic monitoring, and surgery when needed. However, some patients continue to experience persistent inflammation, tissue damage, fistulas, or repeated relapse despite conventional treatment.
This is why regenerative medicine has gained attention. Mesenchymal stem cell therapy, also called mesenchymal stromal cell therapy in many scientific settings, is being explored as a supportive cellular approach for selected Crohn’s disease cases. The goal is not to replace gastroenterology care or promise a cure. Instead, stem cell therapy is studied for its potential to influence immune signaling, reduce destructive inflammation, support tissue repair, and create a more balanced healing environment around damaged intestinal or perianal tissue.

Why Crohn’s Disease Is Difficult to Control
Crohn’s disease develops through a complex interaction between genetic susceptibility, immune dysregulation, gut microbiome imbalance, epithelial barrier dysfunction, and environmental triggers. In some patients, genetic factors such as NOD2-related pathways may affect how the immune system recognizes bacteria in the intestine. In others, gut dysbiosis may disturb the normal relationship between protective microbes and the intestinal immune system. When the epithelial barrier becomes more permeable, bacterial products and inflammatory signals can move deeper into the bowel wall, activating immune cells and sustaining chronic inflammation.
This immune activation involves several pathways, including T-helper 1 and T-helper 17 activity, inflammatory cytokines such as TNF-alpha, IL-6, IL-12, and IL-23, macrophage activation, oxidative stress, and impaired regulatory immune control. Over time, repeated inflammation may damage the intestinal wall, reduce nutrient absorption, and contribute to scarring or narrowing of the bowel.
This is why symptom relief does not always equal mucosal healing. A patient may feel better after a flare is controlled, but still carry underlying tissue vulnerability. A major goal in modern Crohn’s management is not only reducing symptoms, but also controlling inflammation deeply enough to reduce complications and protect long-term bowel function.
Where Standard Treatments Help and Where Gaps Remain
Conventional and biologic therapies remain central in Crohn’s disease care. Corticosteroids can rapidly reduce inflammation during acute flares, but they are not designed for long-term maintenance because of metabolic, bone, immune, and hormonal side effects. Immunomodulators and biologic agents can reduce inflammatory activity, yet some patients never respond fully, and others lose response over time.
Surgery can be essential for strictures, obstruction, abscesses, severe bowel damage, or treatment-resistant fistulas. However, surgery removes damaged tissue; it does not remove the underlying immune tendency that caused the disease. This is why recurrence after bowel resection remains an important clinical issue.
The gap is clear: Crohn’s disease is not only an inflammation problem. It is also a tissue repair problem, an immune regulation problem, and a barrier integrity problem. stem cell therapy is being explored because it may address several of these biological layers at the same time.
What Mesenchymal Stem Cells Are
Mesenchymal stem cells are multipotent cells that can be isolated from sources such as bone marrow, adipose tissue, and umbilical cord tissue, including Wharton’s jelly. In clinical research, stem cell therapy are valued less for becoming new intestinal cells directly and more for their paracrine signaling. This means they release bioactive molecules, cytokines, growth factors, extracellular vesicles, and immune-modulating signals that can influence nearby and distant cells.
Umbilical cord-derived stem cell therapy are of particular interest because the tissue can be collected non-invasively after healthy birth, and the cells are generally considered biologically young, highly expandable, and strongly immunomodulatory in laboratory and early clinical research settings. However, cell source matters. Adipose-derived stem cell therapy, bone marrow-derived stem cell therapy, and umbilical cord-derived stem cell therapy are not automatically interchangeable. Processing quality, donor screening, viability, sterility testing, dose, route, and clinical protocol all affect safety and consistency.
How MSC Stem Cell Therapy May Support Crohn’s Disease
- Immune Modulation Without Full Immune Shutdown
One of the most important features of stem cell therapy is their ability to communicate with immune cells. Instead of acting like a conventional immunosuppressive drug that blocks one pathway, stem cell therapy appear to influence several immune networks. Research suggests that MSCs may reduce overactive Th1 and Th17 inflammatory activity while supporting regulatory T cells, or Tregs, which help restore immune tolerance.
In Crohn’s disease, this is relevant because the immune system often behaves as if normal gut bacteria or intestinal contents are threats. By encouraging a more regulated immune response, stem cell therapy may help shift the local environment from ongoing attack toward controlled repair. This does not mean stem cell therapy cure the immune tendency behind Crohn’s disease. It means they are being studied as a way to reduce inflammatory intensity and improve the conditions needed for healing.
- Macrophage Polarization
Macrophages are immune cells that can either worsen inflammation or help resolve it, depending on their state. In active Crohn’s disease, pro-inflammatory M1-like macrophage activity can contribute to tissue injury and cytokine release. MSCs can secrete mediators such as prostaglandin E2 and other anti-inflammatory factors that may encourage macrophages to shift toward a more M2-like reparative profile.
This shift is important because healing requires more than stopping inflammation. Damaged tissue also needs cleanup, new matrix organization, improved blood supply, and signals that guide epithelial repair. A more reparative macrophage environment may help reduce the cycle of injury and incomplete healing that contributes to chronic intestinal damage.
- Supporting Epithelial Barrier Repair
The intestinal lining acts as a selective barrier. It allows nutrients to pass while helping prevent harmful microbes, toxins, and inflammatory triggers from entering deeper tissue layers. In Crohn’s disease, this barrier can become disrupted. Tight junctions between epithelial cells may weaken, and inflammatory injury can make the lining more permeable.
Stem cell therapy secrete growth-supporting signals such as transforming growth factor-beta, vascular endothelial growth factor, hepatocyte growth factor, and other repair-associated mediators. These signals may support epithelial cell survival, angiogenesis, and tissue remodeling. In theory, a stronger barrier may reduce ongoing immune stimulation and help the intestine move toward a more stable state. This remains an area of active investigation, especially for luminal Crohn’s disease.
Delivery Routes: Systemic and Local Approaches
The best delivery route depends on the patient’s disease pattern. For luminal Crohn’s disease affecting the small bowel or colon, intravenous infusion is often discussed because it exposes the systemic immune environment to stem cell therapy signaling. IV delivery is being studied for its potential to modulate inflammation throughout the body, although direct “homing” to intestinal lesions should not be overstated because cell distribution and persistence are complex.
For complex perianal fistulas, local injection has the strongest clinical foundation. In this approach, cells are injected around the fistula tract after appropriate surgical preparation, drainage, and closure of the internal opening when indicated. The goal is to concentrate immunomodulatory and repair signals directly around the abnormal tunnel, helping the tissue close in a controlled way.
These two routes should not be confused. A patient with diffuse intestinal inflammation is different from a patient with localized perianal fistulizing disease. Proper case selection, imaging, endoscopic evaluation, infection control, medication history, and gastroenterologist review are essential before any regenerative plan is considered.
What Clinical Evidence Shows
The strongest evidence for stem cell therapy in Crohn’s disease is in complex perianal fistulas, especially treatment-refractory cases. Darvadstrocel, an expanded allogeneic adipose-derived stem cell therapy, became an important milestone because it was developed specifically for local injection in complex perianal fistulas in Crohn’s disease. Earlier clinical trials and real-world studies reported encouraging fistula closure and safety outcomes in selected patients.
However, the evidence picture has become more nuanced. Alofisel, the brand name for darvadstrocel, previously held EU marketing authorization, but the European Commission withdrew that authorization in December 2024 at the request of the marketing authorization holder. EMA stated that no new patients should be treated with Alofisel in the EU after December 13, 2024. Takeda reported that the larger ADMIRE-CD II trial did not meet its primary endpoint, while also noting no new emerging safety signals.
This does not erase the scientific value of stem cell therapy research in Crohn’s disease. It does mean that clinics and healthcare providers must describe the evidence honestly. stem cell therapy for Crohn’s disease should be presented as a developing and carefully selected regenerative option, with the most mature evidence in perianal fistulizing disease and more limited, investigational evidence for broad luminal Crohn’s disease.
Patient Selection and Safety
Not every Crohn’s disease patient is an ideal candidate for stem cell therapy care. A careful evaluation should consider disease location, disease activity, fistula presence, abscess risk, infection status, current medications, nutritional condition, inflammatory markers, colonoscopy findings, MRI pelvis findings when fistulas are present, and previous response to biologics or surgery.
Patients with active uncontrolled infection, undrained abscess, severe malnutrition, unstable systemic illness, or urgent surgical complications may not be suitable until these issues are addressed. For perianal fistulas, drainage and surgical preparation are often as important as the cell product itself. For luminal disease, stem cell therapy should be considered only as part of a broader plan that includes gastroenterology management, monitoring, nutrition, and realistic outcome tracking.
The safety of stem cell therapy depends heavily on cell quality and clinical protocol. Important factors include donor screening, infectious disease testing, sterility testing, endotoxin testing, mycoplasma testing, cell identity, viability, passage number, culture conditions, transport conditions, and documentation. “Stem cells” should never be treated as a generic product. Poorly processed or poorly documented cells create unnecessary risk.
A Balanced Regenerative Perspective
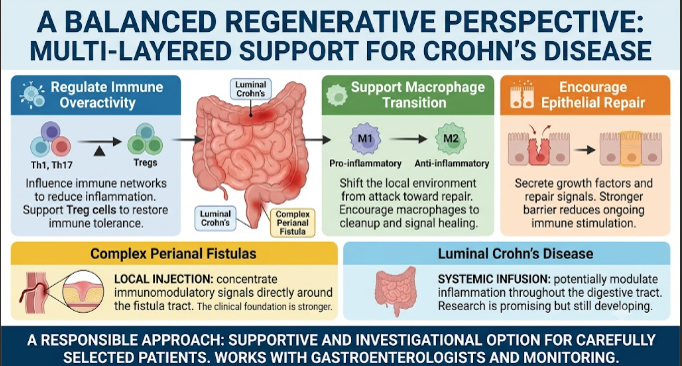
Mesenchymal stem cell therapy represents one of the most interesting areas in regenerative medicine for Crohn’s disease because it addresses more than one biological pathway. It may help regulate immune overactivity, support macrophage transition, encourage epithelial repair, and improve the local healing environment. For complex perianal fistulas, the clinical foundation is stronger. For luminal Crohn’s disease, research is promising but still developing.
The most responsible way to discuss stem cell therapy is not as a replacement for standard care, but as a supportive and investigational option for carefully selected patients. Crohn’s disease is complex, and no single treatment can solve every layer of the condition. A thoughtful regenerative approach should work with gastroenterologists, imaging, laboratory testing, nutrition, infection control, and long-term monitoring.
For patients living with Crohn’s disease, the goal is not simply to suppress symptoms for a short period. The deeper goal is to reduce destructive inflammation, protect intestinal structure, improve daily function, and support the body’s ability to heal where healing is still possible. stem cell therapy is not a dramatic promise, but when presented honestly and used carefully, it may become part of a more complete conversation about the future of IBD care.