

- Stem Cell Therapy for Chronic Skin Wounds: Understanding Diabetic Ulcers, Poor Circulation, and Regenerative Support
Chronic skin wounds are not simply wounds that take a little longer to close. They often mean that the body’s normal repair process is stuck. A wound may remain open because of diabetes, poor blood circulation, repeated pressure, nerve damage, infection, immune dysfunction, nutritional problems, or long-term inflammation.
For patients, a non-healing wound can become more than a skin problem. It can affect walking, sleep, hygiene, clothing, confidence, travel, and daily independence. In serious cases, chronic ulcers may increase the risk of infection, hospitalization, tissue loss, or amputation.
This is why many patients search for stem cell therapy for chronic skin wounds, especially when dressings, antibiotics, wound cleaning, debridement, or standard wound care have not produced enough progress.
The responsible way to discuss stem cell therapy is not to promise instant wound closure. A more accurate explanation is that mesenchymal stem cells, especially UC-MSC stem cell therapy, are being studied for their potential to support the wound microenvironment, inflammation balance, angiogenesis signaling, and tissue repair communication.
2.Why Chronic Skin Wounds Become Difficult to Heal
- A Wound Can Become Stuck in the Inflammatory Phase
Normal wound healing is a coordinated process. The body controls bleeding, clears damaged tissue, manages inflammation, builds new tissue, forms blood vessels, and remodels the skin over time.
In chronic wounds, this sequence may become disrupted. The wound may remain inflamed, poorly oxygenated, infected, under pressure, or unable to build healthy tissue.
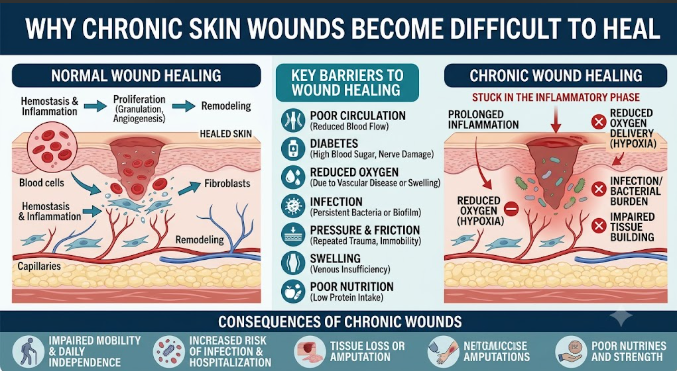
Common barriers to wound healing include:
- Poor circulation
- Diabetes-related nerve and blood vessel changes
- Reduced oxygen delivery
- Infection or bacterial burden
- Pressure or repeated friction
- Swelling or venous insufficiency
- Poor nutrition or low protein intake
- Smoking or vascular disease
- Uncontrolled blood sugar
- Reduced mobility
A dressing can protect the surface, but deeper healing often requires correcting the biological and mechanical reasons why the wound is not progressing.
- Common Types of Chronic Skin Ulcers
- The Cause of the Wound Changes the Treatment Plan
Not all chronic ulcers behave the same way. A responsible wound care plan should identify the wound type before considering regenerative support.
Diabetic foot ulcers often involve neuropathy, pressure, impaired circulation, immune dysfunction, and slow tissue repair. These wounds require offloading, blood sugar control, infection monitoring, vascular assessment, and regular follow-up.
Venous leg ulcers are often linked to poor venous return and swelling in the lower legs. Compression therapy, edema control, and circulation review may be important.
Pressure ulcers develop when prolonged pressure reduces blood flow to the skin and deeper tissues. Repositioning, pressure relief, nutrition support, and infection prevention are central.
Arterial ulcers are related to poor blood supply. These wounds require vascular evaluation because tissue cannot heal properly without enough oxygen and nutrients.
This is why stem cell therapy should not be offered as a one-size-fits-all wound treatment.
- What UC-MSC Stem Cell Therapy Means in Wound Care
- Supportive Signaling, Not Simple Skin Replacement
A common misconception is that stem cells directly become new skin and close the wound by themselves. In modern MSC research, the more accurate explanation is supportive biological signaling.
Umbilical cord-derived mesenchymal stem cells, or UC-MSC stem cell therapy, are studied because they may release bioactive signals, including cytokines, growth factors, extracellular vesicles, and other paracrine mediators. These signals may influence how surrounding cells behave during repair.
For chronic skin wounds, UC-MSC stem cell therapy are being investigated for their potential role in:
- Modulating excessive inflammation
- Supporting angiogenesis, or new blood vessel signaling
- Encouraging fibroblast and keratinocyte activity
- Supporting collagen and extracellular matrix organization
- Improving the local tissue repair environment
- Supporting immune balance around the wound
- Helping shift the wound away from a prolonged inflammatory state
This does not mean stem cell therapy guarantees complete wound closure. It means MSC-related signaling is being studied as one possible supportive part of advanced wound care.
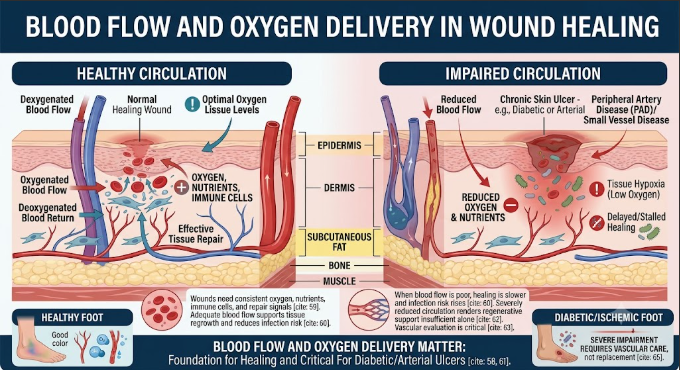
- Why Blood Flow and Oxygen Delivery Matter
- A Wound Cannot Repair Well Without Circulation
A wound needs oxygen, nutrients, immune cells, and repair signals. When blood flow is poor, healing becomes slower and infection risk may increase.
This is especially important in diabetic foot ulcers and arterial ulcers. If circulation is severely reduced, regenerative support alone is not enough. The patient may need vascular evaluation, blood flow testing, and standard medical treatment before any advanced wound option is considered.
One reason stem cell therapy is being studied in wound care is the potential of stem cell therapy signaling to support angiogenesis and tissue repair communication. However, this should not be described as a replacement for vascular care.
- Stem Cell Therapy Should Work With Standard Wound Care
- Regenerative Support Cannot Replace the Basics
Chronic wound care depends on fundamentals. Stem cell therapy should be discussed only as supportive care, not as a replacement for proper wound management.
A complete wound plan may include:
- Wound cleaning and appropriate dressing
- Debridement when medically needed
- Infection assessment and treatment
- Pressure offloading in diabetic foot ulcers
- Vascular assessment
- Blood sugar management
- Nutrition and protein support
- Swelling or edema control
- Pain management
- Pressure relief and mobility planning
- Regular wound measurement and follow-up
For diabetic foot ulcers, international wound guidelines continue to emphasize offloading, infection control, vascular assessment, wound care, and multidisciplinary management as key parts of care.
- Patient Selection: Who Needs Careful Review Before Treatment?
- Not Every Wound Is Ready for Regenerative Support
Before considering stem cell therapy, a physician should review the patient’s wound and general health carefully.
Important questions include:
- What caused the wound?
- How long has it been open?
- Is there infection?
- Is there enough blood flow?
- Is the wound under pressure?
- Is blood sugar controlled?
- Has vascular disease been checked?
- Is nutrition adequate?
- Is there kidney disease or immune suppression?
- Has standard wound care been optimized?
- What treatments have already been tried?
Patients with active infection, severe vascular disease, uncontrolled diabetes, unstable medical conditions, or urgent surgical needs may require standard medical treatment first.
- What Patients Should Ask Before Stem Cell Therapy for Wounds
- Safety and Transparency Should Come First
Patients should ask clear questions before treatment:
- What type of stem cells are used?
- Are they UC-MSCs?
- How are donors screened?
- Are sterility, endotoxin, and viability tests available?
- Who supervises the treatment?
- How is the wound assessed before therapy?
- Will infection and circulation be checked?
- How will progress be measured?
- What results should not be promised?
Patients should be cautious of any clinic that guarantees wound closure, promises to prevent amputation, or offers regenerative treatment without reviewing infection status, circulation, diabetes control, and wound cause.
- How Progress Should Be Measured
- Wound Healing Should Be Tracked Objectively
Wound improvement should be monitored with practical and visible markers, not vague impressions.
A proper follow-up plan may track:
- Wound size
- Wound depth
- Drainage level
- Odor or infection signs
- Pain level
- Granulation tissue quality
- Skin edge condition
- Blood flow status
- Blood sugar control
- Walking or pressure exposure
- Dressing frequency
- Time to partial or complete closure
Photographs can be useful, but they should be taken consistently with similar lighting, distance, angle, and measurement reference.
- Realistic Expectations for Stem Cell Therapy and Chronic Wounds
- Chronic Wounds Often Need Time and Multiple Layers of Care
A chronic wound may have been open for weeks, months, or even longer. Healing can be slow if pressure, infection, blood sugar, nutrition, or circulation remain poorly controlled.
Stem cell therapy may be explored as supportive regenerative care for selected patients, but outcomes can vary depending on wound type, size, depth, duration, vascular status, infection status, diabetes control, age, mobility, and overall health.
The most honest goal is not “one injection and the wound disappears.” The better goal is to improve the wound environment so the body has a better chance to move through the healing process.
Conclusion: A Better Way to Discuss Stem Cell Therapy for Chronic Skin Wounds
Stem cell therapy for chronic skin wounds should be discussed with both hope and caution. UC-MSC stem cell therapy are being studied because of their potential roles in paracrine signaling, inflammation balance, angiogenesis support, extracellular matrix remodeling, and tissue repair communication.
But chronic wound care must remain grounded in medical fundamentals: infection control, vascular assessment, pressure offloading, blood sugar management, nutrition, debridement when appropriate, and consistent follow-up.
For patients with diabetic ulcers, venous ulcers, pressure wounds, or other long-standing skin ulcers, the best approach is not a dramatic promise. It is a careful, physician-led plan that identifies why the wound is not healing and uses regenerative medicine only as a supportive part of a broader wound care strategy.
FAQ: Stem Cell Therapy for Chronic Skin Wounds
- Can stem cell therapy heal chronic skin wounds completely?
Stem cell therapy should not be presented as a guaranteed cure for chronic wounds. It is being studied as supportive regenerative care, and outcomes depend on wound type, blood flow, infection status, diabetes control, nutrition, and overall health.
- Why are UC-MSCs studied for wound healing?
UC-MSCs may release bioactive signals that influence inflammation, angiogenesis, fibroblast activity, keratinocyte activity, extracellular matrix remodeling, and tissue repair communication.
- Is stem cell therapy enough for diabetic foot ulcers?
No. Diabetic foot ulcers require standard wound care, pressure offloading, infection management, blood sugar control, vascular assessment, and follow-up. Stem cell therapy should only be considered as supportive care when medically appropriate.
- What should be checked before treatment?
Patients should be assessed for wound cause, infection, blood circulation, diabetes control, pressure exposure, nutrition status, kidney function, vascular disease, and overall medical stability.
- How should wound healing be monitored?
Progress should be monitored using wound size, depth, drainage, pain, infection signs, granulation tissue, skin edge condition, photographs, and regular clinical follow-up.