

Autism spectrum disorder (ASD) is a heterogeneous neurodevelopmental disorder that can impact communication, sensory, sleep, motor planning, emotional and cognition regulation as well as attention and social engagements and functional daily adaptive function. As autism can vary tremendously from child to child, you may have one child who struggles primarily with sensory sensitivity and another who needs support regarding speech or behavioral regulation or self-care (e.g., bathing themselves) or participation in learning.
And this is why, numerous families search for stem cell therapy for autism, UC-MSC Thailand and OT Therapy for autism as part of complete supportive care plan. Questioning not whether stem cells alone can “treat autism” but whether a physician-supervised regenerative approach plus structured OT could combine into a more sensible supportive mix for some children is the responsible question.
Even so, the wording has to be medically circumspect. Regenerative medicine therapeutics are not FDA-approved for the treatment of autism, and must be presented as investigational, not a cure or alternative to accepted developmental therapeutics. The FDA says that regenerative medicine therapies have not been approved or authorized to treat autism.
This leads to why UC-MSCs are mentioned in autism research
UC-MSCs (Umblilicle Cord-derived Mesenchymal Stem/stromal Cells) are interested in regenerative medicines as they may generate bioactive molecules including growth factors and cytokines, extracellular vesicles and other signaling molecules. The role proposed for them has mainly been limited to paracrine signaling, immune modulation, inflammatory balance and supportive communication with the local tissue.
In particular, UC-MSCs do not get investigated in the context of autism because they just “turn into fresh brain cells.” In more academic terms, it is possible that the factors they secrete may act on biological pathways discussed in studies relating to ASD (including immune dysregulation, neuroinflammation, oxidative stress, gut-brain interaction and cellular stress signaling). Recent reviews reiterate the limitations of the clinical evidence and the need for systematic evaluations before any stem cell-based therapy for ASD can be regarded as standard care, That is why autism stem cell therapy should not be cast as developmental treatment, but rather investigational supportive care instead.
The Importance of OT Therapy in Autism Treatment
Occupational therapy is about finding ways to help children participate more successfully in the daily life. Support utilized by OT for Autistic children sensory processing body awareness fine motor skills emotional regulation feeding routines and habits shifting focus handwriting play skills self-care attention functional independence
OT for autistic children is applied to self-care, emotional regulation, alertness, handwriting, organization, social participation (and more), and even hobbies and play. It also illustrates how support with sensory processing can help children whose initial reaction is often to become calmer and more focused.
There remains much work to explore sensory-based and sensory integration interventions for autistic children in the current literature. Sensory integration approaches may improve behavior and daily performance of children with ASD.
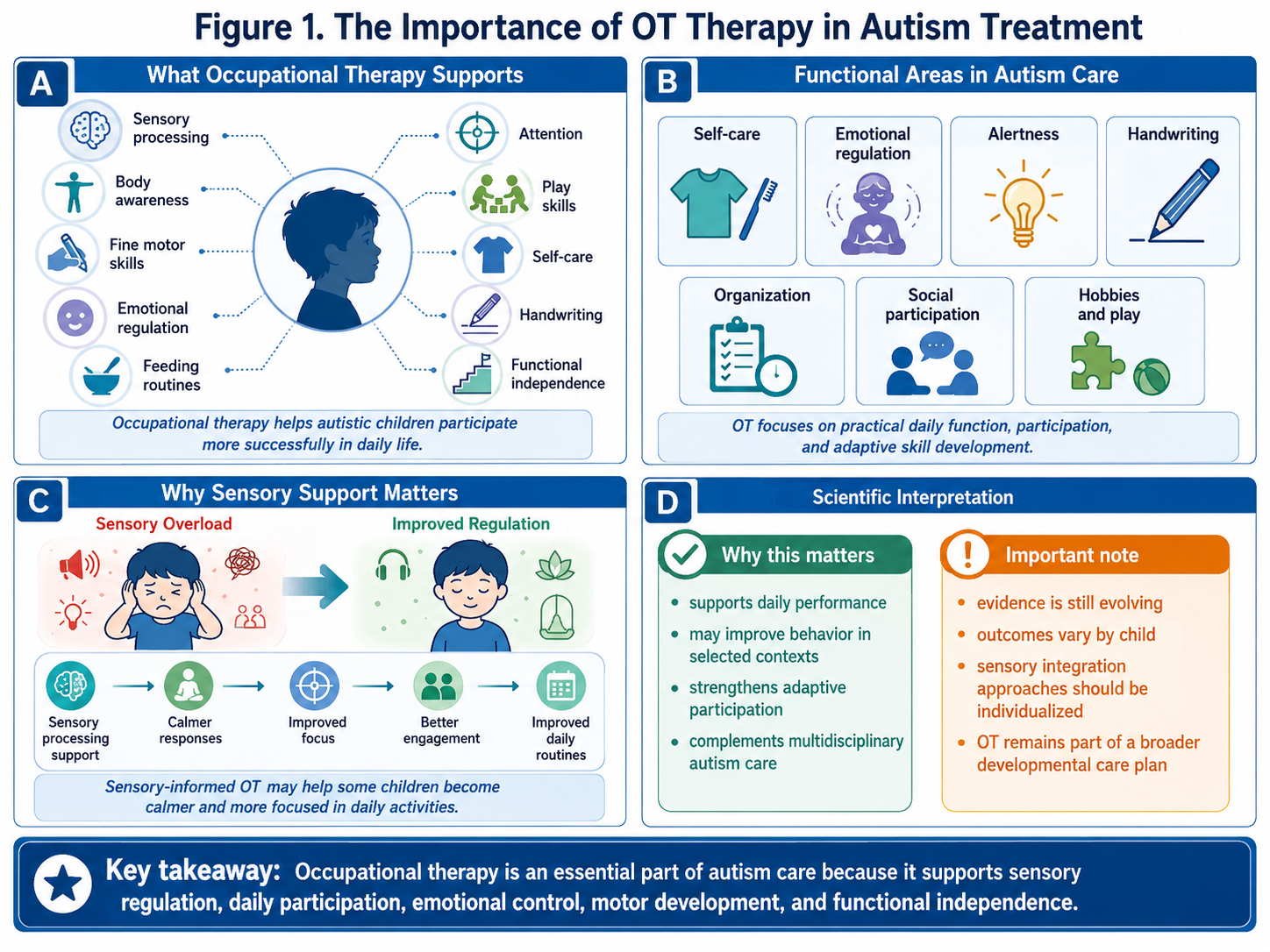
Figure 1: The Importance of Occupational Therapy in Autism Treatment
The Logical Case for Supposting Both Stem Cells and OT
Stem cell program not really like OT therapy. Hence, the potential clinical relevance of this combination may be greater than offering each as a monotherapy.
The Biological Environment: A Focus of Stem Cell Support
UC-MSCs are suggested to possibly support immune equilibrium, regulation of inflammation, modulation of oxidative stress and gut-immune-brain communication. These are biological pathways.
OT Therapy: Channeling Support Into Everyday Function
OT is about the practical: being able to (physically) sit longer during lesson time, tolerate sensory input more easily, reduce motor-planning challenges, succeed at dressing or eating skills, become less overwhelmed and have even functional routines.
This combination creates a bridge between biology and behaviour
The biological basis for more complex behaviours and abilities may be innate, but development still requires repetition, practice, structured therapy and at-home or community routines led by family members. However, that potential improvement in attention, regulation and comfort has to be translated into real-world skills through OT.
An example of how a responsible framework might look:
Facility assessment → UC-MSC understudy program → OT appraisal → sensory guideline arranging → functionality skill preparing → caregivers home design → four-week tone supervisor
Embedding stem cells within this structure gives a stronger rationale than presenting them as an end solution.
Daily adaptive function
This is what OT is especially important for it provides the child with structured opportunities to repeat and practice these skills. Shellder, a Bernstein-affiliated company providing unique support as we develop stem cell lines for our research is tailored to the internal biological environment future home, while OT concentrates largely on function, how one behaves and participates.
Why Patient Selection Matters
Regenerative Medicine is an autism, but not every child with autism is the same, and not every child is right for a regenerative medicine program! Things to consider prior to trying UC-MSC Thailand with OT therapy for autism are:
ASD diagnosis
Developmental history
Communication level
Sensory profile
Sleep pattern
Gastrointestinal symptoms
Seizure history
Immune or allergy background
Current medications and supplements
Previous therapy response
OT baseline assessment
Pediatric or neurological review
This assessment provides realistic goals, The targets of intervention can vary depending on the specific child; one may be addressing sleep and sensory issues, while another works on abilities with self-feeding toilet skills, emotional regulation, or classroom participation.
A Better Way For Explaining What The Goal Of It
Investigational regenerative approaches centered on immune and inflammatory signaling (eg, stem cell support) may also be explored as a potential adjunct; whereas occupational therapy (OT), through structured developmental training, offers sensory regulation, adaptive function, and participation in daily life.
This message is much more credible, as it disassociates biological backing from functional treatment.
Conclusion
Stem Cell Support with OT for Autism is a hot topic because families want more holistic care options. Such studies should examine the immunomodulatory, anti-inflammatory, paracrine and tissue-supporting signaling properties of UC-MSCs. OT therapy, in contrast, is still a very relevant area because it enable functioning each day, sensory drive and their level of rest and core motor planning for self-care as per regulation of both suchapeutic interventions between caloricals they assist.
The potential benefit from this combination is that the program is not solely dependent on stem cells. Instead of linking it to biological support, they connect the dots with developmental practice. This may result in a semi-structured, more pragmatic care pathway for some children.
UC-MSCs are still investigational for use in autism, and results can differ. The safest and most ethical option is physician involvement, adequate safety screening, precise cell processing such as concentrated mononuclear cells., patient-centered OT goals derived from clinical reasoning with family support or companionship plus long-term follow-up. In autism care the best model combines science, therapy and functional support without a promise of cure.