

Stem Cell-Based Strategies in Crohn’s Disease: A Patient-Centric Academic Review
Crohn Type 1: Crohns disease), a chronic inflammatory bowel disease that can affect any part of the gastrointestinal (GI) tract. It is a chronic illness that occurs in flares with periods of no signs or symptoms and varies in severity from one person to another. Symptoms are relatively well controlled in some patients but not others, who experience repeated flares of inflammatory activity and debilitating complications such as pain; nutritional problems; and fistulas or strictures which reduces their quality of life. Long-term management of Crohn’s disease usually involves more than just treatment, as the disease occurs in most people with mild and moderate forms over many years.
For many patients, not only is Crohn’s disease a digestive disease. Chronic abdominal pain, diarrhea, fatigue, weight loss or anemia and malabsorption can disrupt work, sleep and social life as well as have an emotional impact. Ongoing disease activity may also represent uncertainty and psychological stress, particularly in those with prior medication changes requiring use of multiple treatments or surgery. This explains, in part, why patients and clinicians keep searching for other treatments that may be more effective, including regenerative and stem cell-based treatment strategies.
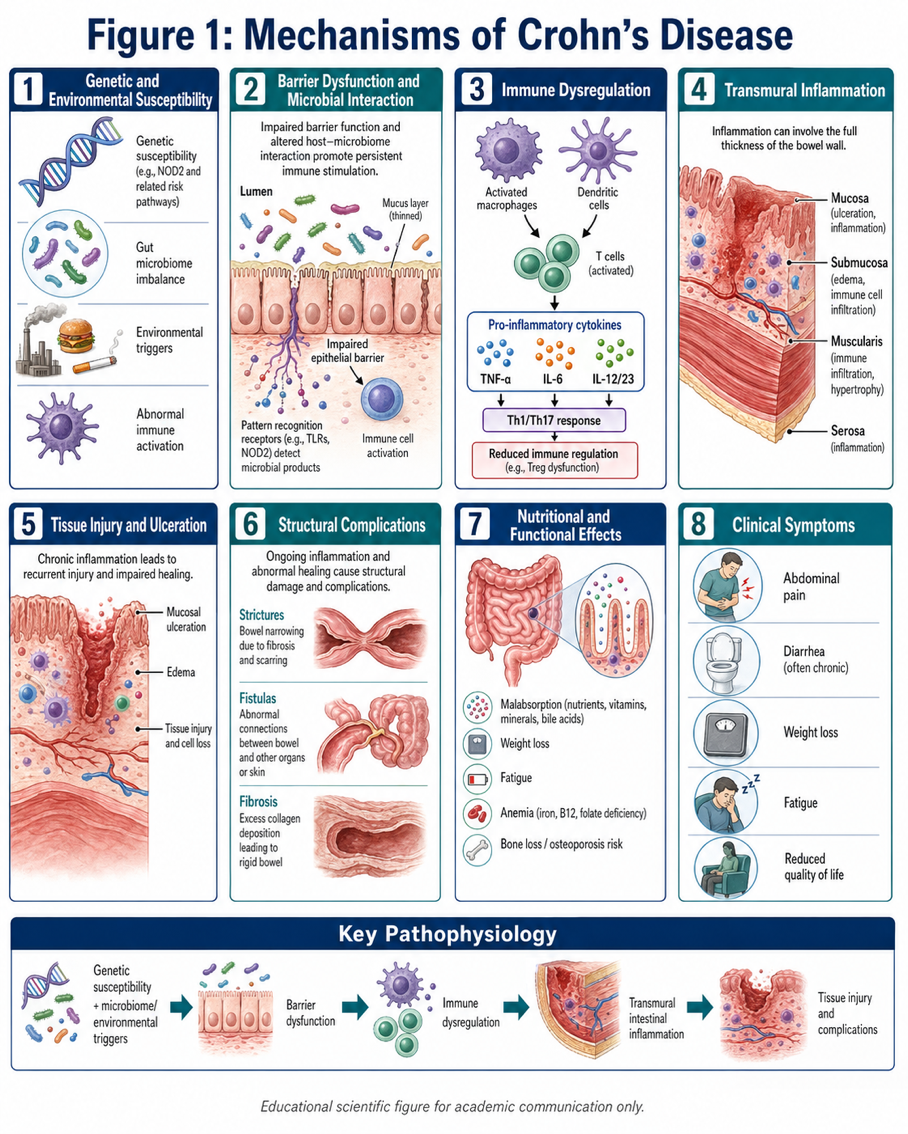
Crohn’s disease is not a single-gene disease. It is widely defined as an abnormal immune response to the intestinal microbiome in a genetically predisposed individual and possibly affected by environmental factors. Rather than curbing its activity to balance the gut bacteria and intestinal contents, the immune system becomes hyperreactive and keeps inflammation alive in bowel wall.
The inflammation in Crohn’s disease is often transmural (through the full thickness of the intestinal wall). This explains why fistulas, strictures and abscesses may occur. At a cellular level, inflammatory pathways with cytokines including tumor necrosis factor-alpha, interleukins, macrophages and T cells lead to recurrent tissue damage. Eventually the bowel develops ulceration, scarring, narrowing, or loss of structural integrity.
Such sustained inflammation may in addition disturb the intestine’s normal nutrient absorption. Consequently, it proceeds to some degree of loss in weight, iron deficiency, vitamin deficiency as well as just common weakness among patients. In more severe disease systemic burden rather than local burdens affect general health and daily function.
Traditional Therapeutic Approaches and Their Limitations
The aim of traditional remedy includes decreasing irritation, reaching remission, and averting complications. Standard medical treatment include corticosteroids for acute flares, immunomodulators, biologic therapies, nutritional support and surgery as required. These therapies remain cornerstones of modern Crohn’s disease treatment and are associated with better outcomes for many patients.
But not every patient responds completely or consistently. That means some treatments respond well at first but then stop working over time. Some can produce dangerous side effects or may be insufficient for patients with complex illness, particularly fistulas and severe structural bowel injury. Sometimes surgery is required, and this delivers vital relief but it does not treat the root condition. This inflammation may come back even after the affected part is removed.
This translates into a battle between disease control, side effects, quality of life and the long-term need to spare bowel from resectioning in treatment decisions among patients. This reality has spurred interest in novel approaches that may promote immune modulation coupled with tissue repair.
Why stem cell-based therapy is still under research?
However, the mechanism of action for stem cells appears to differ from standard immune-suppressing treatment options and is being explored in Crohn’s disease. Mesenchymal stem or stromal cells (MSCs) in particular are known for their immunomodulatory, anti-inflammatory and tissue supporting properties. They are not cells that are explored and investigated as “replacement” cells. They are being investigated instead for their effects on the inflammatory milieu and their ability to modulate pro-healing signals in damaged tissue.
These cells are the subject of research interest as they stimulate immunoregulatory processes that could reduce harmful immune response, direct inflammatory reactivity to a more regulated state, and promote healing of injured mucosa. Several proposed mechanisms include effects on T-cell regulation, macrophage polarization, cytokine signaling and local tissue repair pathways. The situation is particularly acute in Crohn’s disease since this condition reflects immune dysregulation but also involves damage to anatomically important structures within the bowel wall.
However, we must explain this with caution. At this point in time, stem cell-based therapy should be recognized as an experimental or niche option not a one-size-fits-all surrogate for standard treatment. The most important question to patients might not be whether the therapy sounds good (theoretically), but where it would fit within actual clinical care.
Most Probably Relevant to Patients
The best way to think about stem cell-based therapy, from a patient perspective, is based on the goals of treatment. Patients typically want to know if a therapy will improve pain, bowel symptoms, inflammation, fistula healing or nutritional stability or the need for repeated escalation of treatment. They are also interested in whether it is appropriate for their particular disease pattern.
This suggests that in practice such stem cell-based approaches may be more relevant for certain cases over others of Crohn’s disease. The strongest clinical interest has been in challenging fistulizing disease, which tends not to heal completely with traditional treatment. The focus for other patients may still be on standard medical therapy, nutrition, monitoring and complication prevention.
So why is individual assessment important of the basis for treatment decisions — disease location and severity, prior treatment history, complications, nutritional status, and overall health — drives better outcomes for patients than sweeping claims about any single therapy.
A Balanced Clinical Perspective
To many who are living with Crohn’s disease, this will come as no surprise; you start searching for treatments far beyond just controlling the symptoms in the short term. Regenerative medicine is harnessing a new biological way of thinking about chronic inflammation and tissue injury. That possibility is scientifically important. But at the same time unrealistic expectations are best avoided too.
In this context a more responsible description of stem cell-based therapy is the following: it is an actively researched and maturing clinical domain that may confer benefit in select cases, particularly where inflammation and tissue injury are not easily controlled but also does not represent a straightforward or infallible means to be pursued with abandon. Established gastroenterology care encompassing nutritional support, monitoring and prevention of complications should still be considered an integral part of long-term disease management for patients.
Conclusion
Crohn disease is a complex inflammatory disorder that impacts both physiological health and the day-to-day course of life for affected individuals. Although all current treatments are crucial, they don’t solve every clinical conundrum and patients with refractory disease or those who have complicated rheumatic diseases often need alternative treatment options. Stem cell based therapy gained interest because of its possible role to support immune regulation and tissue healing, but needs to be interpreted carefully in the context of mindful medicine.
For patients, it is most helpful to think not about whether one treatment is “better” in general but whether a given approach maps onto the particular kind of disease they have (or suspect), the goals of care and where they are in their treatment course; clear discussion with experienced clinicians still represents by far the most important step in determining what direction next to pursue.