

Cervical spondylosis is a degenerative condition of the neck that affects the cervical spine, including the discs, vertebral joints, ligaments, nerve openings, and sometimes the spinal cord itself. It is commonly described as “neck arthritis” or age-related wear and tear, but the condition is more complex than simple aging. As the cervical discs shrink, lose hydration, or bulge, the body may form bone spurs, ligaments may stiffen, and the spaces around the nerve roots or spinal cord may become narrower. Cervical spondylosis as degeneration of the bones and discs in the neck, which can lead to bulging discs, herniated discs, and bone spurs.
For many patients, cervical spondylosis causes neck stiffness, muscle tightness, headaches, shoulder discomfort, or reduced range of motion. In other cases, the condition may irritate or compress nerve roots, producing pain, numbness, tingling, or weakness that travels into the shoulder, arm, or hand. This is called cervical radiculopathy. In more serious cases, degenerative changes may compress the spinal cord, leading to cervical myelopathy, which can affect walking, hand coordination, balance, and bladder function.
Umbilical cord-derived mesenchymal stem cells, or UC-MSCs, are being studied in regenerative spine medicine because of their potential effects on inflammation, extracellular matrix balance, immune regulation, tissue repair signaling, and the microenvironment around degenerative spinal structures. However, UC-MSC stem cell therapy should not be described as a guaranteed cure for cervical spondylosis. It should not replace urgent spine care when there is spinal cord compression, progressive weakness, or severe neurological impairment. A responsible clinical framework is that UC-MSC stem cell therapy may offer biological support in selected patients after proper imaging review, neurological assessment, and physician-led treatment planning.
Understanding Cervical Spondylosis as a Multi-Structure Disorder
The cervical spine includes seven vertebrae, intervertebral discs, facet joints, ligaments, muscles, nerve roots, and the spinal cord. The cervical region must support the head while allowing rotation, flexion, extension, and fine movement. Because it is highly mobile, the neck is vulnerable to repetitive stress, posture-related overload, disc degeneration, and joint wear.
Cervical spondylosis may involve several structures at once. The intervertebral discs may lose water and height. The annulus fibrosus may develop fissures. The facet joints may become arthritic. The uncovertebral joints may form spurs. The ligamentum flavum or posterior longitudinal ligament may thicken. The foramina, where nerve roots exit the spine, may narrow. These changes can combine to produce neck pain, nerve irritation, or spinal canal narrowing.
This is why cervical spondylosis should not be treated as one uniform diagnosis. A patient with mild disc degeneration and muscle spasm is different from a patient with foraminal stenosis and arm weakness. A patient with neck pain only is different from a patient with spinal cord compression and gait instability. Treatment must match the dominant pain generator and neurological risk.
Neck Pain, Radiculopathy, and Myelopathy Are Not the Same
The first is axial neck pain. This may come from discs, facet joints, ligaments, muscles, posture, or inflammation. Symptoms are usually centered in the neck and may spread to the upper back, shoulder blade, or head.
The second is cervical radiculopathy. This occurs when a cervical nerve root becomes irritated or compressed, often from disc herniation, foraminal stenosis, or bone spurs. AAOS describes cervical radiculopathy as a “pinched nerve” condition in the neck that may cause pain radiating into the shoulder and arm, and treatment may include medication, physical therapy, injections, or surgery when necessary.
The third is cervical myelopathy. This is more serious because it involves spinal cord compression. Symptoms may include hand clumsiness, dropping objects, numbness in both hands, balance difficulty, gait instability, leg stiffness, or bladder changes. A clinical practice guideline for degenerative cervical myelopathy recommends surgical intervention for patients with moderate and severe disease and suggests either surgery or structured rehabilitation for selected mild cases, with surgery recommended if neurological deterioration occurs.
This distinction is essential. UC-MSC stem cell therapy may be discussed as supportive biological care in selected degenerative or inflammatory cases, but it should not delay surgical evaluation when myelopathy or progressive neurological deficit is present.
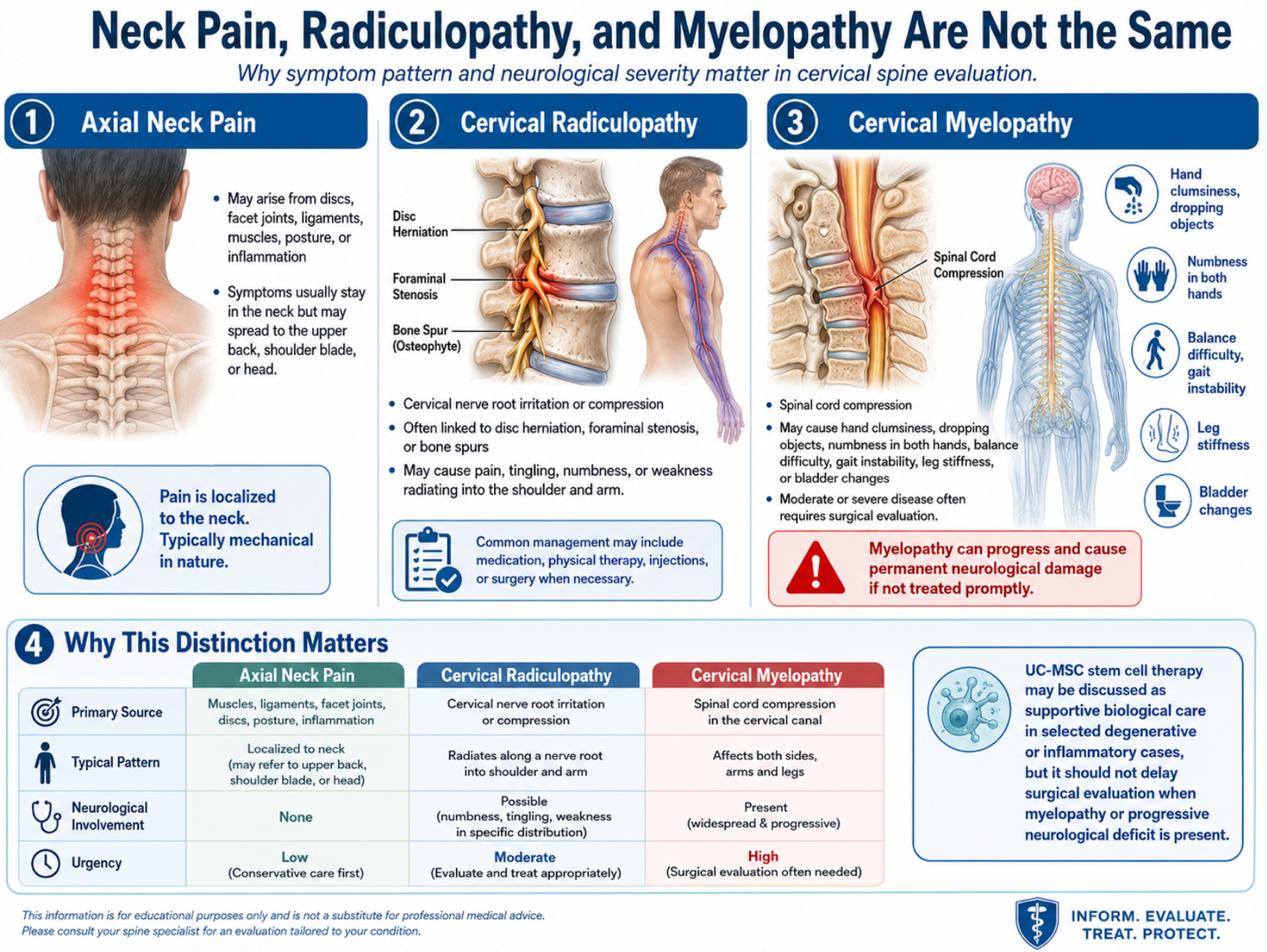
Figure 1: Neck Pain, Cervical Radiculopathy, and Cervical Myelopathy Are Distinct Clinical Conditions
Why Cervical Degeneration Becomes Painful
Degeneration does not always equal pain. Some people have MRI findings such as disc bulging, narrowing, or bone spurs without significant symptoms. HSS notes that wear-and-tear changes may appear on imaging even when a person has no pain or discomfort.
Pain develops when structural degeneration interacts with inflammation, nerve irritation, mechanical overload, muscle guarding, or instability. A dehydrated cervical disc may lose height and increase load on facet joints. A bulging disc may release inflammatory mediators. Bone spurs may narrow the foramina and irritate nerve roots. Stiff ligaments may reduce movement and contribute to canal narrowing. Muscle guarding may develop as a protective response, but over time it can worsen stiffness and pain.
This is why treatment planning should not rely only on the MRI report. The physician must correlate imaging with symptoms, physical examination, neurological findings, and functional limitations.
Standard Treatment and Its Limitations
Most symptomatic cervical spondylosis cases begin with conservative care unless there are red flags. Standard treatment may include physical therapy, posture correction, ergonomic changes, medication, short-term collar use in selected cases, nerve pain medication, anti-inflammatory strategies, or image-guided injections.
However, conservative care may not fully address the biological environment of degeneration. Medication can reduce symptoms but does not rebuild discs. Physical therapy improves strength and movement control but may not directly reduce inflammatory disc signaling. Surgery can decompress nerves or stabilize the spine when needed, but it is not intended to regenerate tissue. This treatment gap explains why regenerative medicine has gained interest.
What Are UC-MSC Stem Cell Therapy?
UC-MSC stem cell therapy are mesenchymal stem or stromal cells derived from Wharton’s jelly of the umbilical cord. They are collected after healthy birth donation and processed under controlled laboratory conditions. In modern regenerative medicine, UC-MSC stem cell therapy are mainly studied as signaling cells, not as simple replacement cells.
Their secreted factors may include cytokines, growth factors, microRNAs, extracellular vesicles, and immune-regulatory proteins. These signals may communicate with immune cells, fibrocartilage-like cells, endothelial cells, and inflamed tissue environments.
For cervical spondylosis, the scientific interest is not that UC-MSC stem cell therapy create a new neck or reverse every bone spur. The more realistic concept is that they may support the local spine microenvironment by influencing inflammation, tissue repair signaling, extracellular matrix balance, and cellular stress responses.
How UC-MSC Stem Cell Therapy May Support Cervical Spondylosis
1. Inflammation Modulation
Inflammation contributes to pain in degenerative spine conditions. Disc injury, facet irritation, and nerve root inflammation may all produce pain signals. UC-MSC stem cell therapy may release factors that help regulate inflammatory cytokines and immune-cell behavior. This may be relevant for patients whose symptoms include inflammatory neck pain, stiffness, or radicular irritation.
2. Disc Microenvironment Support
Cervical discs can degenerate through dehydration, matrix breakdown, annular fissuring, and reduced cellular repair capacity. Reviews of stem cell therapy for degenerative disc disease describe intervertebral disc degeneration as involving matrix changes and inflammation, making it a major research target for regenerative strategies.
UC-MSC stem cell therapy may support repair signaling, but it should not be described as proven disc regrowth. Disc degeneration is structurally complex, and the cervical spine is anatomically sensitive.
3. Facet Joint and Soft-Tissue Support
Cervical facet joints can become arthritic and inflamed, contributing to neck pain and restricted motion. Surrounding ligaments and muscles may also become overloaded. UC-MSC stem cell therapy may be discussed as supportive care for selected degenerative joint or soft-tissue inflammation, but the exact target should be determined by examination and imaging.
4. Nerve Root Irritation Support
When nerve symptoms are driven partly by inflammation around a compressed or irritated nerve root, biological support may be considered in selected cases. However, if the nerve is severely compressed by a large disc herniation, bone spur, or foraminal collapse, mechanical decompression may be required. UC-MSC stem cell therapy cannot reliably remove structural compression.
5. Rehabilitation Tolerance
Pain can prevent proper rehabilitation. If biological therapy helps reduce inflammatory stress in selected patients, the patient may better tolerate neck stabilization exercises, deep cervical flexor strengthening, scapular control, mobility work, and ergonomic correction. Long-term success depends heavily on movement quality and posture habits.
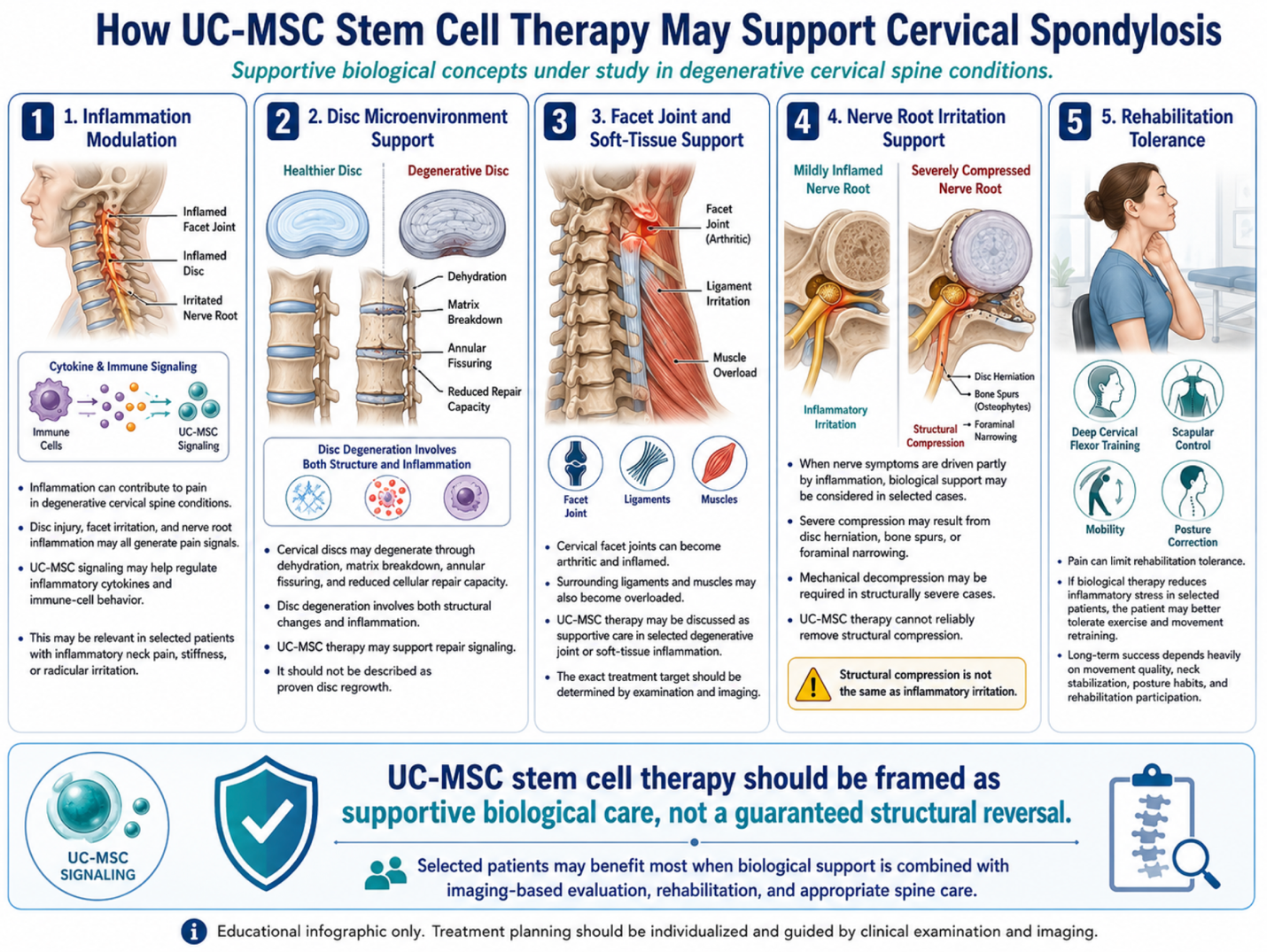
Figure 1: UC-MSC Therapy for Cervical Spine Degeneration: Inflammation, Disc, and Nerve Support
Patient Selection: Who May Be Considered?
UC-MSC stem cell therapy may be considered for selected patients with cervical spondylosis who have chronic neck pain, early-to-moderate disc degeneration, inflammatory cervical facet pain, persistent symptoms despite conservative care, or mild radicular symptoms without progressive neurological loss.
It may be less appropriate for patients with moderate or severe cervical myelopathy, spinal cord signal changes, progressive arm or leg weakness, severe canal stenosis, unstable spondylolisthesis, fracture, infection, tumor, or major deformity. These patients require spine specialist evaluation. In myelopathy, delay can increase the risk of long-term neurological impairment.
A responsible program should review MRI findings, X-rays if needed, neurological examination, pain distribution, arm symptoms, reflex changes, hand function, balance, previous treatments, medications, and rehabilitation history.
Image-Guided Planning Matters
The cervical spine contains the spinal cord, nerve roots, vertebral arteries, and many sensitive structures. Any interventional treatment around the cervical spine requires careful anatomical planning and appropriate imaging guidance. The target may be the disc, facet joint, ligamentous region, epidural space, or surrounding soft tissues depending on the physician’s assessment.
UC-MSC stem cell therapy should not be presented as one standard injection for all neck problems. A patient with C5-C6 foraminal stenosis may need a different plan from a patient with C3-C4 facet arthritis or C6-C7 discogenic pain. Diagnosis determines the treatment target.
Safety, Quality Control, and Regulation
For UC-MSC stem cell therapy, cell quality is essential. Important factors include donor screening, infectious disease testing, sterility testing, endotoxin testing, cell identity markers, viability, culture conditions, transport timing, and physician monitoring. A high cell number alone does not prove safety or efficacy.
Regulatory language should also be careful. The FDA states that regenerative medicine therapies are not approved in the United States for orthopedic conditions, including disc disease, back pain, neck pain, and shoulder pain. Regulations differ by country, but this reinforces the need for transparent claims, proper documentation, and realistic medical counseling.
Realistic Expectations After UC-MSC Therapy
UC-MSC stem cell therapy should not be described as instant cervical spine regeneration. Cervical spondylosis usually develops over years. Bone spurs, severe stenosis, advanced disc collapse, and spinal cord compression cannot be assumed to reverse with cell therapy.
Realistic goals may include reducing inflammatory pain, improving neck mobility, supporting tissue repair signaling, improving tolerance for rehabilitation, reducing stiffness, and helping selected patients maintain function. Progress should be measured with pain scores, neck disability index, range of motion, arm symptoms, sleep quality, medication use, neurological findings, and functional tolerance.
Patients should continue physical therapy, posture correction, ergonomic adjustment, strengthening, weight management, sleep support, and physician follow-up. Regenerative therapy works best when it is part of a complete spine preservation plan.
Conclusion
Cervical spondylosis is a multi-structure degenerative condition involving discs, facet joints, bone spurs, ligaments, nerve roots, muscles, and sometimes the spinal cord. Because symptoms may range from mild neck stiffness to cervical radiculopathy or myelopathy, treatment must be guided by accurate diagnosis and neurological risk assessment.
UC-MSC stem cell therapy is being studied as supportive regenerative medicine because of its potential effects on inflammation regulation, paracrine signaling, extracellular matrix support, tissue repair communication, and the degenerative spine microenvironment. It should not be promoted as a cure, a guaranteed disc-regeneration method, or a replacement for surgery when spinal cord compression is present.
For patients considering stem cell therapy for cervical spondylosis in Thailand, the safest approach begins with MRI-based evaluation, physician-led diagnosis, neurological screening, high-quality UC-MSC preparation, transparent safety testing, realistic expectations, and structured rehabilitation. Responsible regenerative neck care is not about promising a new spine. It is about supporting selected biological pathways while protecting the patient from delayed treatment when serious neurological signs are present.
FAQ
Can UC-MSC therapy cure cervical spondylosis?
No. UC-MSC therapy should not be described as a cure. It may support inflammation regulation and tissue repair signaling in selected patients, but it cannot be guaranteed to reverse disc collapse, bone spurs, or spinal stenosis.
Is cervical spondylosis the same as cervical radiculopathy?
No. Cervical spondylosis refers to degenerative changes in the neck. Cervical radiculopathy occurs when a nerve root is irritated or compressed, causing symptoms such as arm pain, numbness, tingling, or weakness.
When is UC-MSC therapy not appropriate?
UC-MSC therapy may not be appropriate when there is moderate or severe cervical myelopathy, progressive weakness, spinal cord compression, infection, tumor, fracture, severe instability, or urgent surgical indication.
What tests should be reviewed before treatment?
Important tests include cervical MRI, X-ray when needed, neurological examination, reflex testing, arm strength, sensory assessment, pain pattern, previous treatment history, and physician evaluation.
Do patients still need physiotherapy after UC-MSC therapy?
Yes. Rehabilitation remains important. Neck stabilization, posture correction, scapular strengthening, mobility training, and ergonomic changes all support long-term cervical spine health.