

Persistent Long COVID Symptoms can feel confusing because they rarely follow one simple pattern. Some patients experience severe fatigue, brain fog, shortness of breath, chest discomfort, dizziness, sleep disruption, muscle pain, post-exertional worsening, palpitations, or reduced stamina months after the original infection. Routine tests may appear acceptable, yet the patient still feels far from recovered.
This is why interest in stem cell therapy Thailand for Persistent Long COVID Symptoms continues to grow. Patients are not only asking for symptom relief. Many want to understand whether lingering inflammation, microvascular stress, immune activation, endothelial dysfunction, or abnormal clotting signals may be contributing to their condition.
A responsible discussion must be careful. DFPP and UC-MSC stem cell therapy should not be promoted as cures for Long COVID. The more accurate conversation is about physician-led assessment, blood filtering in selected cases, inflammatory burden reduction, and supportive regenerative signaling.
Long COVID Is a Multisystem Condition
Long COVID is not one disease with one mechanism. It may involve immune dysregulation, viral persistence hypotheses, autonomic nervous system disturbance, endothelial dysfunction, mitochondrial stress, microvascular impairment, mast cell activation, or post-infectious inflammation. Different patients may have different dominant drivers.
This explains why one person mainly has fatigue and brain fog, while another has breathlessness, palpitations, chest tightness, digestive symptoms, or pain. A single protocol cannot be assumed to fit every patient.
A high-quality stem cell therapy Thailand program should begin with full assessment, not immediate treatment. Medical history, infection timeline, vaccination history, symptom pattern, exertional tolerance, cardiovascular status, clotting risk, inflammatory markers, medications, and red flags should be reviewed carefully.
Why Microclots Are Being Discussed
Microclots are one of the more debated areas in Long COVID research. Some studies have reported fibrinaloid or amyloid-like clotting material in blood samples from patients with Long COVID. The hypothesis is that these abnormal clot-related particles may interfere with microcirculation, oxygen delivery, and inflammatory signaling.
This idea may help explain why some patients feel exhausted even after small activity, or why cognitive symptoms can feel worse after exertion. If tissues are not receiving oxygen and nutrients efficiently, the body may struggle to recover after normal stress.
However, microclots are not yet a universal diagnostic marker or proven treatment target for every patient. The concept remains under investigation, and patients should be cautious of clinics that claim microclot removal guarantees recovery.
Cytokines and Persistent Immune Activation
Cytokines are immune signaling molecules. During infection, cytokines help coordinate defense and repair. But when inflammatory signaling remains active after the acute infection has passed, the body may stay in a prolonged alarm state.
Persistent cytokine activity may contribute to fatigue, sleep disruption, pain sensitivity, endothelial irritation, brain fog, and slower recovery. This is why Long COVID is often discussed as both an immune and vascular condition.
The goal is not to suppress the immune system blindly. The goal is to identify whether the patient has an inflammatory burden that may be clinically relevant and whether reducing that burden may support recovery.
How DFPP Enters the Long COVID Conversation
DFPP, or double filtration plasmapheresis, is a blood purification method that separates plasma and passes it through a secondary filter to remove selected larger molecules before returning filtered components to circulation.
In Persistent Long COVID Symptoms, DFPP may be discussed because some patients may have circulating inflammatory mediators, immune complexes, abnormal proteins, lipid-related particles, or clot-associated factors that contribute to systemic burden. In theory, reducing selected circulating factors may help create a less inflammatory and less microvascularly stressed environment.
This does not mean DFPP is appropriate for everyone with Long COVID. It is a medical procedure that requires physician assessment, safety screening, and clear indication. Patients with bleeding risk, severe anemia, unstable cardiovascular disease, active infection, or complex medication use need careful review.
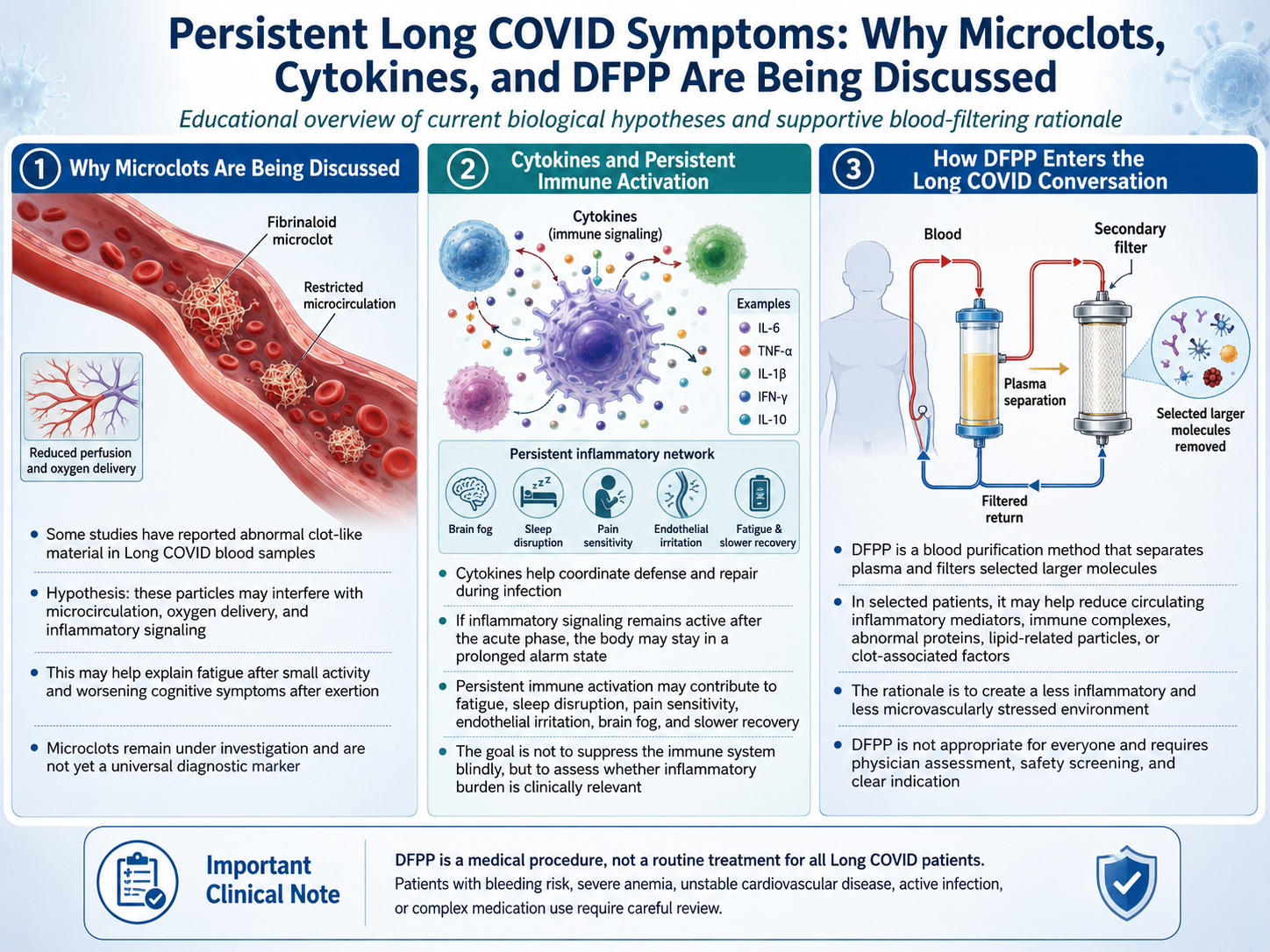
Figure 1: Stem Cell Therapy Thailand for Persistent Long COVID Symptoms: Microclots, Cytokines, and DFPP Support
Why UC-MSC Stem Cell Are Discussed After Blood Filtering
UC-MSCs, or umbilical cord-derived mesenchymal stem cells, are studied for paracrine and immunomodulatory signaling. Their interest is not that they directly repair every organ affected by Long COVID. The more realistic mechanism is communication.
UC-MSC stem cell therapy may release cytokines, growth factors, extracellular vesicles, and other bioactive signals that influence inflammation balance, oxidative stress response, endothelial communication, angiogenesis, and tissue repair pathways.
In a staged model, DFPP may be discussed first to reduce selected circulating burden. UC-MSC stem cell therapy may then be considered for supportive regenerative signaling. The goal is not to force recovery, but to support a more favorable biological environment for repair.
Why Sequencing Matters
Sequencing matters because regenerative support does not happen in isolation. If the internal environment remains highly inflammatory, oxidative, or microvascularly impaired, the body may have less capacity to respond.
The logic is simple: first reduce unnecessary circulating burden where medically appropriate, then support immune regulation, vascular communication, and tissue recovery. This staged approach is not a guarantee. It is a biological rationale that must be individualized.
Standard Long COVID Care Still Matters
Long COVID care should remain grounded in medical evaluation. Patients may need cardiology review, pulmonary testing, neurological assessment, autonomic testing, rehabilitation planning, pacing guidance, sleep support, nutrition, medication review, and mental health support.
Patients with chest pain, fainting, severe shortness of breath, new neurological weakness, oxygen desaturation, or rapidly worsening symptoms need urgent medical evaluation rather than elective regenerative treatment.
Final Perspective
Trapping microclots and cytokines is a useful way to explain one possible biological rationale behind DFPP and UC-MSC stem cell therapy for Persistent Long COVID Symptoms. But the science must be communicated honestly.
Stem cell therapy Thailand may offer a supportive regenerative conversation for selected patients when combined with careful assessment and, where appropriate, blood filtering strategies. DFPP may help reduce selected circulating burden, while UC-MSC stem cell therapy may support immunomodulatory and paracrine signaling.
The strongest approach is physician-led, safety-first, and realistic: identify the dominant drivers, reduce inflammatory and vascular stress where appropriate, and integrate regenerative support only when medically suitable.