

Psoriatic Arthritis is not just some joint pain that occurs in a person with psoriasis. A chronic, immune-mediated inflammatory disease, it can involve the joints and tendons, ligaments of the skin and nails, spine (spondylitis), energy levels, and ability to perform daily activities. It tenders to notice warning signs like swollen fingers, stiffness in the morning fingers or other joints, heel pain, back discomfort, nail changes and fatigue disproportionate to visible skin disease.
This is the reason why people are getting increasingly more interested by stem cell therapy Thailand for Psoriatic Arthritis. Most of the patients are not just looking for relief from pain. They are wondering whether a more broadly regenerative support of the inflammatory burden in behind disease might be possible.
A responsible response has to have the clarity. There is no rationale for marketing UC-MSC stem cell therapy on the basis that it fully cures Psoriatic Arthritis and in no way should be intended to replace rheumatology care, DMARDs, biologics or physician-directed anti-inflammatory treatment when clinically indicated. The more accurate discussion scientifically is one of immunomodulation, inflammatory signaling, tissue repair environment, and supportive regenerative care for select patients.
Psoriatic Arthritis Is More Than a Pain Problem
Pain killers may help ease the symptoms, but cannot account for or dictate the biology of Psoriatic Arthritis. The pathological immune response in the disease has been shown to promote inflammation in the joints and entheses, which are the sites where tendons and ligaments attach to bone.
That is why during disease, patients might exhibit different patterns. There are people with palmar synovitis also having small joints in the hands eg. Some have knee, ankle or foot involvement. Some go on to develop dactylitis, a condition causing diffuse swelling in one or more finger (s) and/or toe (s). Others, suffer with axial symptoms involving the spine or sacroiliac joints.
That visible hurt is just the top layer. In there, inflammatory mediators and immune cells might keep on finding a way to alter how the tissue feels or functions — irritation, firmness, swelling, exhaustion, long haul gamble of joint inflammation.
Why Inflammatory Burden Matters
The inflammatory burden is defined as the entire biological weight generated by continuous immune activation. In Psoriatic Arthritis, this burden can exceed the painful joint. It affects skin flares, and tendon pain as well as metabolic health, cardiovascular risk, sleep quality and energy.
This is why so many patients with mild joint swelling still feel tired. Immune activity depletes biological resources over time. It may hold the body in a chronic low-level state of alarm, promoting slower recovery and increasing pain sensitivity.
A stem cell therapy Thailand program of quality should not be framing Psoriatic Arthritis as merely “wear and tear” illness. They should understand the immunologically driven nature of disease and the requirement for team-delivered care.
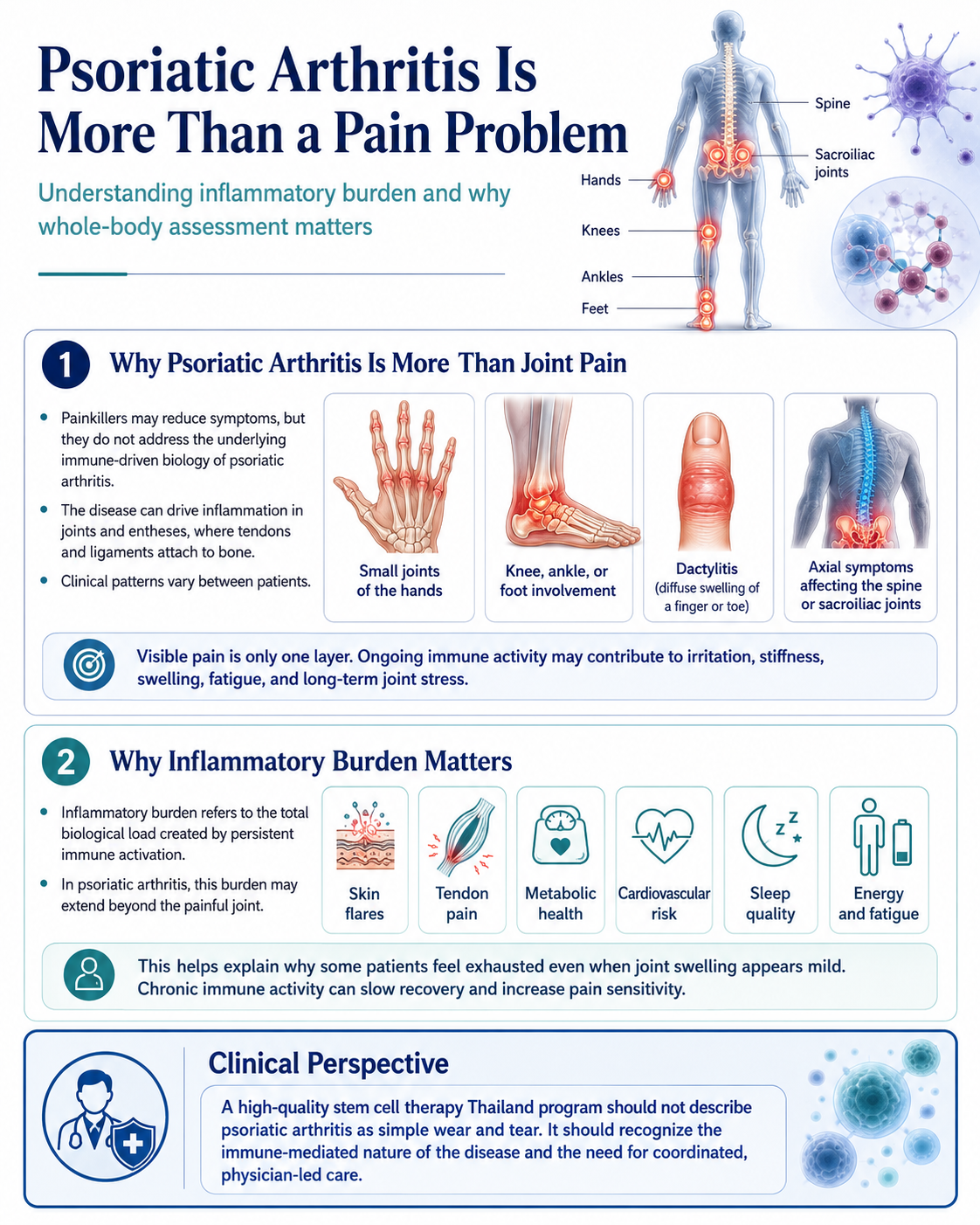
Figure 1: Systemic Inflammatory Burden in Psoriatic Arthritis and Whole-Body Clinical Assessment
Where UC-MSC Stem Cell Enter the Scientific Conversation
The umbilical cord-derived mesenchymal stem cells (UC-MSCs) are the focus of regenerative medicine research due to their immunomodulatory and paracrine signaling abilities. What they really want is not to actually become new joint cartilage or wipe out autoimmune disease. Cell-to-cell communication is the more realistic mechanism.
This includes releasing bioactive molecules, cytokines, growth factors, and extracellular vesicles that could alter local inflammatory signaling pathways or modify the behavior of surrounding immune cells; respond to increased oxidative stress; influence angiogenesis; promote tissue repair communication.
This is relevant to Psoriatic Arthritis as there is immune dysregulation within the disease process. While, UC-MSC stem cells-based support does not intend to turn off the immune system entirely. It is sought to investigate whether biological signaling may assist in a regulated inflammatory environment.
Immunomodulation Is Not the Same as Immune Suppression
The word immunomodulation is important. Immune suppression broadly lower immune activity. Immunomodulation refers to the process of directing immune responses towards more appropriate balanced outcomes.
Psoriatic Patients Do Not Have Autoimmune system Working. What they have to be is an immune system that becomes less misdeveloped and less chronically inflammatory. The separation is important, because the body still requires immune protection against infection and other threats.
The research of stem cells is fascinating for many reasons since stem cells likely interact with immune pathways relevant to T-cell activity, macrophage behavior, cytokine signaling, and inflammation resolution. But the specific clinical outcome may differ according to disease stage, medications, grade of inflammation and health of patients.
Why Standard Psoriatic Arthritis Treatment Still Matters
With Modern Psoriatic Arthritis treatment, so much has changed. Rheumatologists may choose conventional DMARDs, biologics targeting pathways such as TNF, IL-17 or IL-23 and targeted oral therapies depending on the disease pattern and risk profile of each individual patient. RDs aim to suppress inflammation, control symptoms and joint damage, and improve quality of life.
Stem cell therapy is not supposed to compete with these therapies. It should complement rather than replace standard medical care, and so is a responsible regenerative medicine approach.
Medical coordination is crucial, especially for patients already on biologics or immune-modifying therapy. Infection risk, immune status, timing of medications, blood tests and physician oversight should factor in any regenerative protocol.
What a Stem Cell Therapy Thailand Program Should Assess
Clinical assessment is a prerequisite before talking about stem cells therapy for Psoriatic Arthritis. Two physicians trained abstracted diagnosis history — disease duration (years), body surface area (BSA) involvement, total joint count (TJC), skin severity score/patient global assessment, nail involvement, enthesitis and dactylitis counts, axial symptoms; current medications including biologic history and steroid use; comorbidity/history of infections/autoimmune diseases/blood tests/imaging when available.
Your requirements for the patient were as specific too. Is it priority relief of pain, stiffness, swelling, fatigue, mobility, skin activity or recovery after flare? Metrics and response are hard to assess if there is no clarity of objectives.
It would also demonstrate scientific responsibility in discussing aspects of cell source, donor screening, sterility testing, viability, route of administration / dose planning and monitoring and limitations.
The Role of Regenerative Support in Joint and Tissue Health
In Psoriatic Arthritis, inflammation can affect the joint lining, tendon attachments, soft tissues, and surrounding structures. Over time, repeated inflammatory activity may contribute to pain, stiffness, reduced mobility, and tissue stress.
stem cells therapy -based support may be considered for its potential role in modulating inflammatory signaling and supporting tissue repair communication. This does not mean it can reverse established joint damage or guarantee disease control. Rather, it may be discussed as one supportive layer within a broader physician-led plan.
Rehabilitation, nutrition, weight control, sleep, stress reduction, and metabolic monitoring also matter. Psoriatic Arthritis often interacts with cardiovascular and metabolic risk, so whole-body care is more appropriate than focusing only on painful joints.
Safety and Realistic Expectations
Patients should be cautious of any clinic claiming to cure Psoriatic Arthritis, stop all flares, or replace biologic medication with stem cells. These claims are not medically responsible.
Realistic goals may include supporting inflammation balance, reducing systemic burden, improving recovery capacity, and complementing standard care in selected patients. Outcomes vary, and response should be monitored over time through symptoms, function, flare frequency, medication needs, blood markers when appropriate, and quality of life.
Final Perspective
Psoriasis Arthritis, there is more than just pain. It is an inflamed autoimmune disorder that targets the skin, joints, tendons, spine, energy level and long-term health. So this is why more patients are looking for stem cell therapy Thailand as part of a much larger discussion on inflammatory burden and regenerative support?
ASCs represent an important scientific avenue in immune modulation and paracrine signaling but only if the data are presented appropriately. They are not a miracle cure and cannot replace rheumatology care.
We look at the future of PsA treatment as more personalised combinations of biologic medicine, lifestyle support, rehabilitation, metabolic care and regenerative medicine. The best way is definitely NOT just moving off painkillers. It is knowing the immune milieu underlying the pain and delivering medical precision care to an entire person.