

Let’s bust a major myth right out of the gate. Most people look at knee osteoarthritis (OA) as a simple mechanical issue like a car tire wearing down until it’s running on the rim. We call it “wear and tear,” and we assume the fix is either lubricating the joint or replacing the whole hinge.
But medicine has moved past this primitive mechanical view.
Knee OA is actually a complex, biochemically active whole-joint disease. It’s an inflammatory fire inside a living ecosystem. This is exactly why many patients are now looking beyond traditional pain meds and considering Umbilical Cord-Derived Mesenchymal Stem Cells (UC-MSCs) in medical hubs like Bangkok and Phuket.
But before we look at what these cells can do, we need to understand what they cannot do. No serious medical professional will tell you that a cell injection is a magic eraser that instantly rebuilds a shredded joint.
The real science is much more interesting. It’s about supportive signaling.
The Knee Joint as a Stressed Ecosystem
If you want to understand why your knee hurts, you have to look at the whole picture. It is never just about worn cartilage. When osteoarthritis takes hold, every single layer of the joint capsule gets dragged into the fight:
The Synovial Lining: This inner membrane becomes chronically inflamed (synovitis), turning the joint fluid into a toxic cocktail of inflammatory waste.
The Subchondral Bone: The bone directly beneath your cartilage begins to harden, alter its shape, and sprout painful bone spurs (osteophytes).
The Soft Tissue: Menisci fray, and ligaments stretch thin under altered, uneven mechanical loading.
This deep tissue complexity explains a phenomenon that trips up many patients: scans often lie about actual pain.
You can put two patients in an MRI machine; one might show severe cartilage loss but only feel a dull ache, while another with moderate changes struggles to climb a flight of stairs. Why? Because pain is driven by the local biochemical environment and cellular stress, not just the physical structural gap.
The Inflammatory Burden: What Really Drives the Pain
Inside an arthritic knee, the molecular environment is dominated by a destructive biological cascade. Two main inflammatory cytokines cell-signaling proteins called (Interleukin-1 Beta) and (Tumor Necrosis Factor-Alpha) act like cellular saboteurs. They order local cells to produce matrix metalloproteinases (MMPs), which are enzymes that actively chew away at the remaining cartilage matrix.
| The Old Mechanical View | The Modern Biological Paradigm |
| Cartilage is just passive, inert shock-absorbing padding. | The joint is an active, responsive biological ecosystem. |
| Pain is caused solely by physical friction and thinning structural layers. | Pain is heavily driven by chemical irritation and IL-1β / TNF-α signaling. |
| The only logical endpoint for advanced decay is a joint replacement. | The goal is to modulate the microenvironment and calm localized inflammation. |
To stop this breakdown, you don’t just need a physical cushion. You need to flip the biochemical switch from destruction to homeostatic balance.
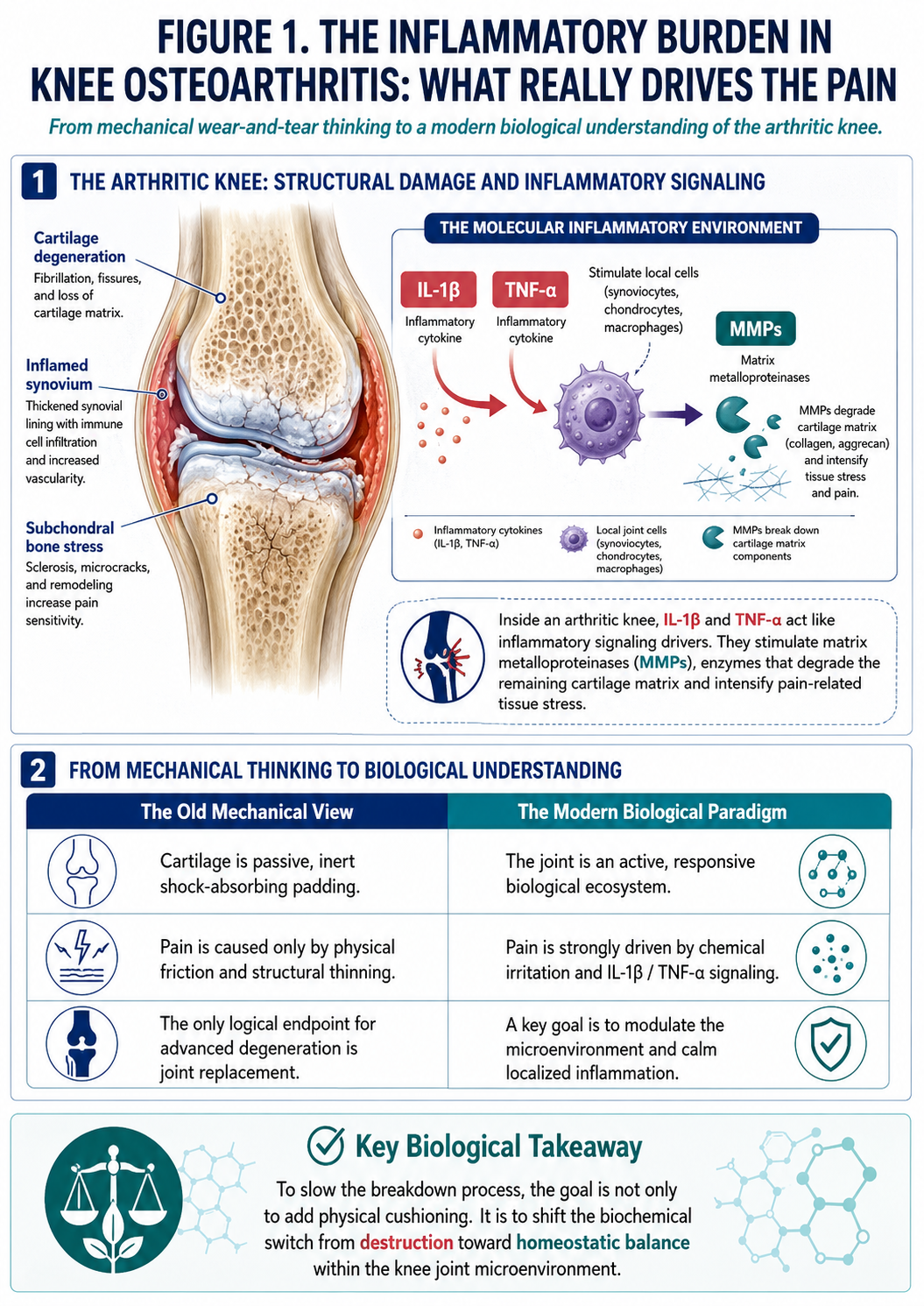
Figure 1: Biological Drivers of Pain in Knee Osteoarthritis: IL-1β, TNF-α, Matrix Metalloproteinases, and the Joint Inflammatory Microenvironment
Enter UC-MSC stem cell : Cell Replacement vs. The Paracrine Secretome
Here is where the massive internet confusion lies. Many clinics advertise stem cells as a way to “grow brand-new cartilage.”
The scientific reality: Injected mesenchymal cells do not permanently attach themselves to your bone and magically transform into fresh hyaline cartilage overnight. That is a myth.
Instead, UC-MSC stem cell work through a mechanism called paracrine signaling. Think of them as localized, highly adaptive biochemical factories. Once introduced into the synovial fluid, they read the inflammatory signals of the joint and release a massive counter-measure known as the cellular secretome.
This secretome matrix contains:
Anti-Inflammatory Cytokines: High concentrations of and designed to block the destructive pathways of .
Trophic Growth Factors: Compounds like that signal surrounding tissue cells to survive, adapt, and stop the self-destruction cycle.
Targeted Exosomes: Microscopic lipid bubbles filled with regulatory microRNA that merge with local joint cells, essentially reprogramming them away from inflammation and toward tissue preservation.
Why Wharton’s Jelly?
When looking at cell options in Thailand, you will generally face a choice between autologous cells (taken from your own bone marrow or fat) and allogeneic cells (derived from newborn umbilical cord tissue, specifically Wharton’s Jelly).
Wharton’s Jelly UC-MSC stem cell hold a massive biological edge: cellular youth.
Adult stem cells carry the biological age, metabolic stress, and environmental wear of the patient. Newborn UC-MSC stem cell have zero cellular age, much higher replication capacity, and a far more robust secretome profile. Because they are immunoprivileged meaning they don’t express the standard surface markers that trigger host immune rejection your body accepts their signaling without a fight. Plus, using donor tissue means you skip the painful bone marrow harvest or liposuction entirely.
Setting Realistic Guardrails in Thailand
Thailand has established itself as an international hub for advanced regenerative research, with specialized centers across Bangkok operating under strict Advanced Therapy Medicinal Product (ATMP) frameworks. However, a safe medical journey requires looking closely at the details.
Before you agree to any protocol, you must demand a verified laboratory analysis certificate from the clinic. You need to verify three hard metrics:
Cell Viability: Are more than 80-90% of the cells alive and active at the time of the procedure?
Sterility: Has the batch cleared all tests for microbial contaminants, mycoplasma, and endotoxins? (Endotoxins are bacterial cell-wall remnants that can trigger severe joint flare-ups if left in the mix).
Mechanical Realism: Does the clinic emphasize physical rehab?
That last point is non-negotiable. No biological signal can fix a knee that is being crushed by bad biomechanics. True joint support requires a dual-track strategy: using UC-MSC stem cell signaling to calm the internal chemical fire, while simultaneously executing a targeted kinetic chain rehabilitation program (strengthening the quadriceps, hamstrings, and hip stabilizers) to lift the physical load off the joint matrix.