

Stem Cell Therapy for Type 2 Diabetes Mellitus: Metabolic Readiness Beyond Blood Sugar
Blood sugar in the end is centre stage for super patients with type 2 diabetes mellitus. This means at every appointment, you end up talking about HbA1c, fasting glucose and insulin: the medication or diet. However, diabetes is not just about glucose. This is a systemic metabolic disease characterized by insulin resistance, chronic inflammation and oxidative stress, hepatic steatosis (fatty liver), endothelial dysfunction/arterial stiffness visceral fatness pancreatic beta-cell exhaustion mechanistic observation which may modulate genes according to diet/concurrent diseases with long-term complication risk.
This is why increasing attention has been paid to stem-cell-research and therapy. Patients are asking whether one therapy lowers glucose. They want to understand if the internal metabolic environment of the body can become more responsive, less inflamed and primed for repair.
Metabolic readiness — a good way to have the conversation surrounding this.
Diabetes and the Meaning of Metabolic Readiness
Metabolic readiness simply indicates that your organism is now much more biologically prepared to respond favorably, both in terms of treatment and lifestyle change as well as tissue repair and vascular protection. In type 2 diabetes mellitus, poor metabolic preparedness may manifest as chronic inflammation, elevated oxidative stress markers and accessibility to oxygen for mobilization in servicing the body (circulation), low energy levels even with improvements elicited by dietary or exercise interventions and reduced ability to sucrose metabolism through impairment of glycolytic/insulin signal reception across sensitivities leading possibly even also premetabolic states called an accelerated glucose disposition potential that renders positive adaptations from taking glycemic burden loads more difficult.
Why this is useful, because two patients with the same HbA1c could have different biology on the inside. Someone can be insulin resistant and have fatty liver. One might be more beta-cell exhausted. Other could have vascular complications or chronic inflammation. We should shape treatment around this kind of biology, not one numeric value in isolation.
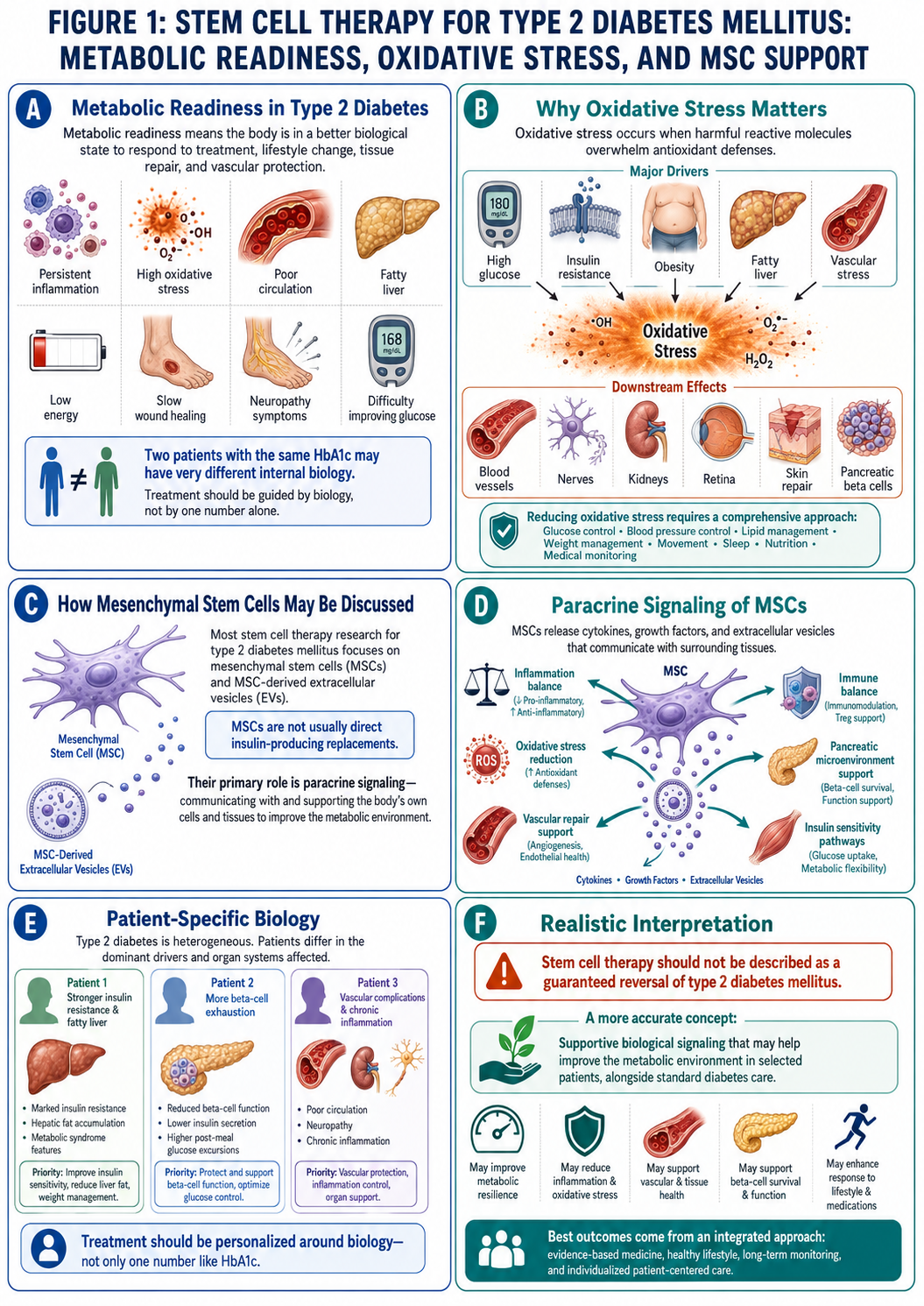
Figure 1: Proposed Supportive Mechanisms of Mesenchymal Stem Cell Therapy in Type 2 Diabetes Mellitus: Oxidative Stress Modulation, Vascular Support, and Metabolic Microenvironment Regulation
Why Oxidative Stress Matters
Oxidative stress occurs when these reactive molecules over-run antioxidant defenses of the body. Elevated glucose levels, insulin resistance, obesity and a fatty liver as well as vascular stress may all contribute to enhanced oxidative damage in type 2 diabetes mellitus.
In the long term, it is likely that oxidative stress influences blood vessels, nerves (neuropathy), kidneys (nephropathy and ESRD [end stage renal disease]), retina (“retinopathy”), skin repair and pancreatic beta cells. It is a reason that allows the complications of diabetes to progress even if at this point everything does not feel strong.
It is not just one supplement, or one injection that will lower oxidative stress. Requires controlling glucose, managing blood pressure and lipids, maintaining a proper weight, movement or activity/rest balance along with appropriate sleep hygiene/management of circadian rhythm/nutrition for metabolic support/trials/proper medical monitoring.
Mesenchymal stem cells might be talked about as follows
The great part of research dealing with stem cell therapy for type 2 diabetes mellitus focuses on mesenchymal types (MSCs) or MSC stem cell-derived extracellular vesicles. Because MSC stem cell are not considered to be direct insulin-producing cell replacements for Type 2 diabetics. Rather, they are studied through paracrine signalling.
MSC stem cell are capable of paracrine signaling and hence they can secrete cytokines, growth factors, extracellular vesicles as well as other molecules to communicate with adjacent tissues. These signals are being applied to diabetes research for possible modulation of pathways such as inflammation, oxidative stress, vascular repair and immune balance in addition to pancreatic microenvironment support mechanisms or insulin sensitivity responses.
A responsible explanation is important. Do NOT label as “a one shot type 2 diabetes mellitus reversal with stem cell therapy.” A more accurate concept for joint anabolic treatment is supportive biological signaling that could improve the metabolic milieu in otherwise appropriate patients.
What Research Suggests So Far
MSC stem cell and MSC-derived exosome research for T2DM are still in their infancy but promising. Reviews cite putative mechanisms involving modulation of inflammation, reduction of oxidative stress, protection of pancreatic beta-cell and improvement in insulin sensitivity. Nonetheless, clinical evidence is still based on small studies with heterogeneous sources of cells and different routes of administration or dosing schemes over a short follow-up.
So patients need to beware of clinics that offer diabetes cure, stop medications or ensure HbA1c normalization.
What Patients Need to Verify Before Treatment
Patients should also have a complete metabolic evaluation prior to weighing options for stem cell therapy. This might include HbA1c, fasting glucose, fasting insulin, C-peptide level if appropriate, lipid profile; liver function tests (e.g., alanine aminotransferase and aspartate aminotransferase); renal urea or plasma creatinine concentrations to estimate kidney functional indices with urine albumin-to-creatinine ratio calculation for monitoring of microalbuminurea blood pressure measurements statistics weight waist circumference neuropathy assessment questioning wound history eye screening medication history cardiovascular risk
C-peptide may be useful in determining whether the pancreas is still producing insulin. It can really add a new dimension to the treatment conversation.
Standard Diabetes Care Must Continue
With type 2 diabetes mellitus, the best evidence is still that of standard care: meal prescription, physical activity promotion as well as weight control; blood glucose monitoring when indicated with anti-diabetic drugs if necessary including oral agents and insulin support to enhance glycaemic goals; management of hypertension or dyslipidaemia and routine footcare along those clinical parameters.
This, along with lifestyle and weight-loss interventions that can improve glycemia in them (and may help some patients attain true remission) should not be interpreted as stem cell therapy being a cure for diabetes.
Conclusion
The notion of stem cell therapy for T2DM needs to be recognized as an experimental and adjunctive discipline, addressing metabolic preparedness, oxidative stress control, inflammation stabilization along with endothelial vascular support and tissue microenvironment regulation.
Never chase a miracle reversal if you want the best. To establish a safer metabolic basis, leverage endocrinology-based care and propose regenerative approaches only with realistic expectations shaped by sound biomedical screening.