

Parkinson’s disease is no longer discussed only as a movement disorder. For patients and families, it is a daily condition that affects walking, tremor, stiffness, sleep, mood, digestion, speech, energy, balance, and confidence. Many people begin with medications that work well at first. Over time, however, the response may become less predictable. “On” and “off” periods may appear. Tremor may become harder to control. Balance and freezing may become more stressful. This is often when families start searching for a stem cell clinic, Parkinson’s disease support, and the latest stem cell trial information.
The growing interest is understandable. Parkinson’s disease is characterized by progressive neurodegeneration of the brain, particularly in areas controlling motor function due to loss of dopamine-producing neurons. It would be natural for any patient with a disease connected to the loss of one or another cell type to ask if some sort of stem-cell product could replace that particular role. The answer, however, must be cautious. Stem cell science has come a long way in Parkinson’s disease, but not all stem cells are the same, and not every clinic-based program is equivalent to what constitutes an appropriately conducted, regulated clinical trial.
A responsible stem cell clinic should explain both sides: the excitement of real scientific progress and the limits of what is currently proven.
Why Parkinson’s Disease Is a Major Focus in Regenerative Medicine
Due to the partly cell–type–specific biology of Parkinson’s disease, it has emerged as a key neuroscience target for regenerative medicine. In contrast to neurodegenerative diseases that affect the brain very diffusely, there is a clear connection between Parkinson’s disease and loss of dopaminergic neurons. Dopaminergic neurons: These create dopamine, a type of neurotransmitter related to movement regulation, coordination, and motivational states.
This is why stem cell trial research has focused heavily on dopaminergic neuron replacement. The idea is not simply to “boost the brain,” but to place carefully prepared dopamine-producing precursor cells into the brain region affected by Parkinson’s disease. In advanced research settings, these cells may be derived from embryonic stem cells or induced pluripotent stem cells, then directed in the laboratory toward a dopamine neuron lineage.
That is very different from a general wellness injection. It is highly specialized, surgical, regulated, and still being studied.
The Difference Between Cell Replacement and Supportive Cell Therapy
When patients search online, they may see many types of stem cell therapy described under one name. This creates confusion. In Parkinson’s disease, there are at least two major concerns.
The first is cell replacement therapy. Such drug discovery programs are known as short- and long-term projects that introduce a stem cell trial-like approach, wherein Scientists generate dopaminergic neuron progenitor cells for direct transplantation into the brain. These studies are intended to determine whether new dopamine-producing cells can survive in the human brain, integrate into neural circuitry, and alleviate motor symptoms.
Second is supportive regenerative therapy using mesenchymal stem cells, also known as MSC. Less emphasis is placed on replacing neurons with MSCs, and more on their paracrine effects. So, they do emit biological signals that can modulate inflammation and immune equilibrium in the body through their communication with various cellular circuits, as well as play a role in preventing oxidative stress, supporting tissue repair by communicating with different types of cells, and affecting cell stimulus response.
A stem cell clinic should never carelessly mix these two ideas. Dopamine cell replacement trials and MSC-based supportive care are not the same treatment.
What Recent Stem Cell Trial Progress Means
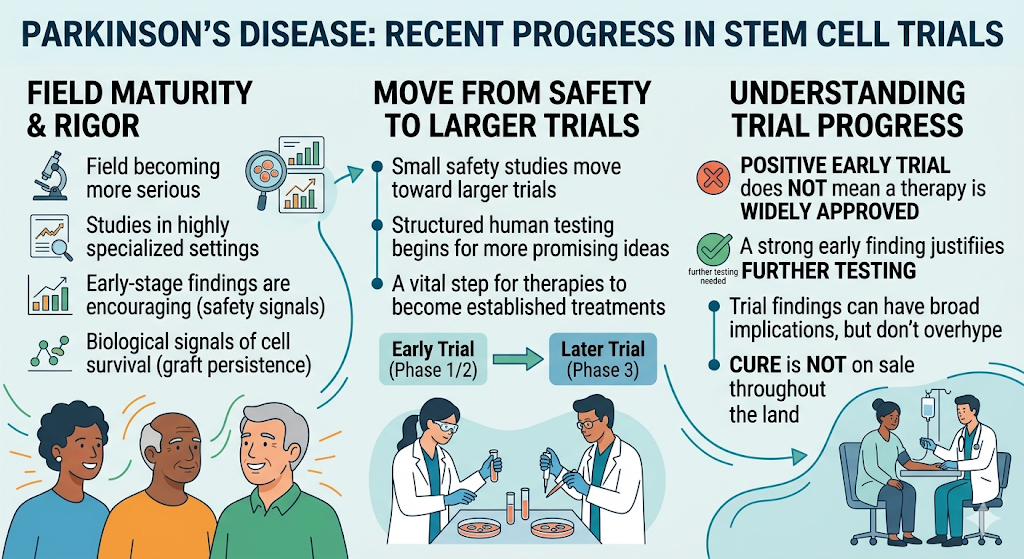
The stem cell trial field in Parkinson’s disease has become more serious in recent years. Early-stage clinical studies using stem cell-derived dopaminergic progenitor cells have reported encouraging safety findings and biological signals suggesting cell survival. Some studies have also reported motor improvement trends, although larger trials are still needed before these therapies can be considered established treatment.
This matters because Parkinson’s disease has had many promising ideas over the years, but only a few have reached the level of structured human testing. The movement from small safety studies toward larger trials shows that the field is maturing. Still, patients should understand what “trial progress” means. A positive early trial does not mean a therapy is widely approved. It means the research is strong enough to justify further testing.
Why Phase 3 Is Important
A Phase 3 stem cell trial is important because it moves beyond early safety questions and begins to test whether the treatment works in a larger, more controlled way. These trials may include sham surgery controls, strict eligibility criteria, standardized outcome measures, long follow-up, and safety monitoring.
For patients, this is a sign of progress, but also a reminder. If a therapy is still in trial, it is not the same as a routine treatment available to everyone. A stem cell clinic that discusses Parkinson’s disease honestly should explain this distinction clearly.
The Role of a Stem Cell Clinic in Parkinson’s Disease Care
A stem cell clinic working with Parkinson’s disease patients should not present regenerative care as a cure. Parkinson’s disease remains a progressive neurological condition. Current standard care includes medication, deep-brain stimulation for selected patients, exercise, physiotherapy, speech therapy, swallowing support, sleep management, nutrition, and long-term neurological follow-up.
Where regenerative care may fit is as a supportive layer. For selected patients, clinic-based stem cell therapy may be discussed as a way to support the body’s repair environment, balance inflammation, mitochondrial stress response, and overall neurological wellness. The goal should be realistic: better support, not guaranteed disease reversal.
A high-quality stem cell clinic should begin with a full review. This may include diagnosis confirmation, disease duration, motor symptoms, non-motor symptoms, medication schedule, “on/off” fluctuations, dyskinesia, fall history, swallowing status, sleep quality, cognitive changes, MRI or DAT scan findings if available, blood tests, and overall medical fitness.
Why Patient Selection Matters
Not every Parkinson’s disease patient is the same. A younger patient with strong medication response and early symptoms is different from a patient with advanced freezing, falls, dementia, swallowing difficulty, and severe autonomic symptoms. Some patients may actually have atypical Parkinsonism, such as multiple system atrophy, progressive supranuclear palsy, or corticobasal syndrome, which may respond differently from classic Parkinson’s disease.
This is why diagnosis matters before any regenerative plan. A responsible clinic should ask for medical records and should be willing to say no when the risk, stage, or diagnosis does not fit the treatment goal.
What Patients Often Hope to Improve
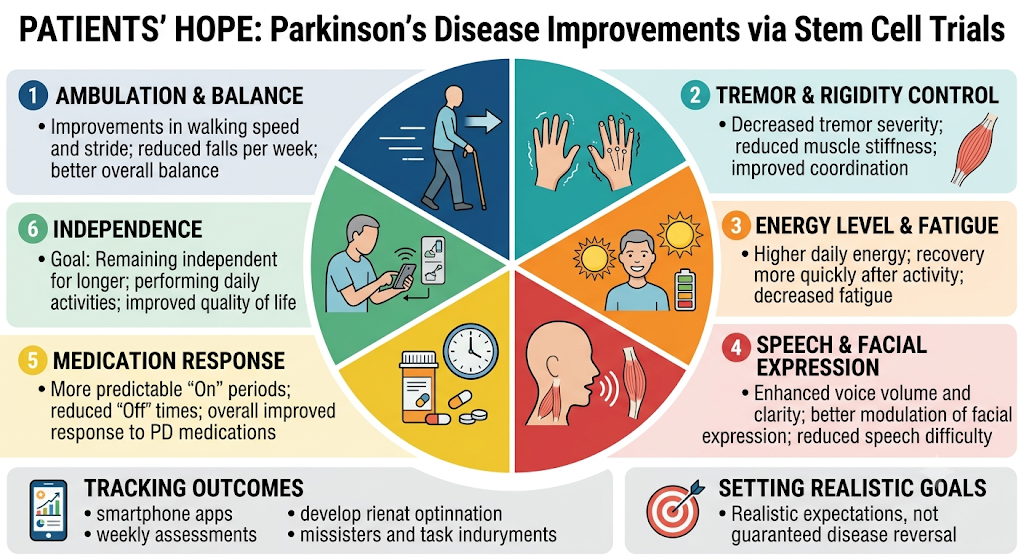
Families typically inquire about ambulation, tremor, balance problems, and stiffness in addition to speech difficulties. Specific wording may vary, sleep changes, or disorders of facial expression, energy level, and response to medications. These are deeply personal goals. Perhaps a patient doesn’t expect perfection: perhaps the goal is simply to walk better, be less fatigued, recover more quickly after therapy, or just remain independent for that much longer.
Such goals should be set before the treatment in a stem cell clinic. Outcomes should be tracked with concrete breadcrumbs: walking speed, number of falls per week, rigidity on a clinical scale (perhaps have the patient submit weekly assessments), tremor severity via smartphone apps or expert visual gaze tracking, and distance walked in one day before they administer medications to their patients.
The Importance of Rehabilitation After Regenerative Care
Stem cell therapy without rehabilitation is incomplete. Parkinson’s disease affects movement habits, posture, balance, muscle coordination, and confidence. Even if regenerative treatment supports the biological environment, the nervous system still needs training.
Exercise is one of the strongest supportive tools in Parkinson’s care. Physiotherapy, balance training, gait work, resistance exercise, stretching, speech therapy, and swallowing support can all help maintain function. A regenerative plan should work with these therapies, not replace them.
Safety Questions Every Patient Should Ask
Before choosing a stem cell clinic, patients should ask what type of cells are used, how they are screened, how sterility is confirmed, how viability is tested, what route of administration is recommended, who performs the procedure, and what monitoring is done afterward.
For Parkinson’s disease, the route matters. Intravenous therapy, intrathecal therapy, and direct brain transplantation are completely different. Direct brain transplantation belongs to specialized clinical trial settings. Intrathecal therapy should only be performed in an appropriate medical facility by qualified physicians. Intravenous MSC therapy is less invasive but should still be medically supervised.
Patients should be cautious of clinics that promise to regenerate dopamine neurons, reverse Parkinson’s disease, stop progression permanently, or produce guaranteed improvement. Parkinson’s disease is too complex for that kind of message.
How to Read Stem Cell Trial News Without Getting Misled
That unit does place some broad parameters on the stem cell trial headlines you may have heard. They see the dopamine-producing cells and brain graft persistence, or they get wind of Phase 3 trials and future pathways for approval, then assume that this cure is already on sale throughout the land. You learn better when you read trial news in a context.
A trial finding may be early but promising. Safety can be demonstrated in small cohorts; larger studies are required to confirm efficacy. Improvements in motor scores are promising, but long-term safety, such as graft behavior, immune response, dyskinesia, and tumor risk, must be monitored together with durability.
They should enable patients to understand research without overhyping it. Good communication builds trust. Overpromising destroys it.
Final Perspective: Hope, Science, and Responsible Care
Parkinson’s disease is a difficult condition because it changes over time and affects more than movement. It affects identity, independence, relationships, and daily rhythm. It is natural for patients and families to look beyond routine medication and ask whether regenerative medicine can help.
Stem cell trial progress in Parkinson’s disease is genuinely important. It shows that the field is moving from theory toward more structured clinical testing. But clinic-based care should remain honest. Stem cell therapy for Parkinson’s disease should be discussed as a supportive and evolving field, not as a guaranteed cure.
The right stem cell clinic should protect patient hope with science. That means careful screening, realistic goals, transparent safety standards, integration with neurological care, and respect for the complexity of Parkinson’s disease.