

Lupus or SLE, are variously described as an autoimmune disease in the common parlance. That explanation, however, remains incomprehensible for many families. So to explain SLE in a more pragmatic manner: the immune system gets confused and starts sending signals shwank to your body.
Rather than protecting the body against infection, it may attack the skin, joints, kidneys and blood vessels to organs like nervous system lungs heart etc. This is why SLE can appear differently from patient to patient. Some population suffer from fatigue and swollen pains, another has skin rashes, kidney inflammation (called glomerulonephritis), blood precursors, hair loss or fever stages that come in waves.
Therefore a description is made focusing on stem cell therapy for SLE in Thailand. It is not a treatment and should never replace rheumatology care. A more rational view of it is that it’s a regenerative medicine adjunct therapy for selected patients, augmenting immune communication and inflammation resolution signals, as well as physical tissue repair signaling.
SLE Is Not Only an Inflammation Problem
Nobody believes that lupus is just (merely) too much inflammation. But SLE is actually more complicated than that. This includes a series of immune miscommunications, which eventually leads to the generation and circulation of autoantibodies as well other pathophysiological factors such immune complexes, type I interferon activation, B cell–T cell imbalance, complement system involvement in circulation and tissues at risk for developing vascular stress leading into tissue inflammation.
This is important for families, because SLE is not like a common allergy or passing sickness. A chronic immune regulation disorder optimised. Some pathways may not be well regulated and others can become over-activated, while flare-ups are characterized by an erratic immune system.
And that is why the aim of treatment isn’t simply to reduce symptoms. The more underlying objective is to help modulate disease activity, organ protection and reduce flares alongside the exposure 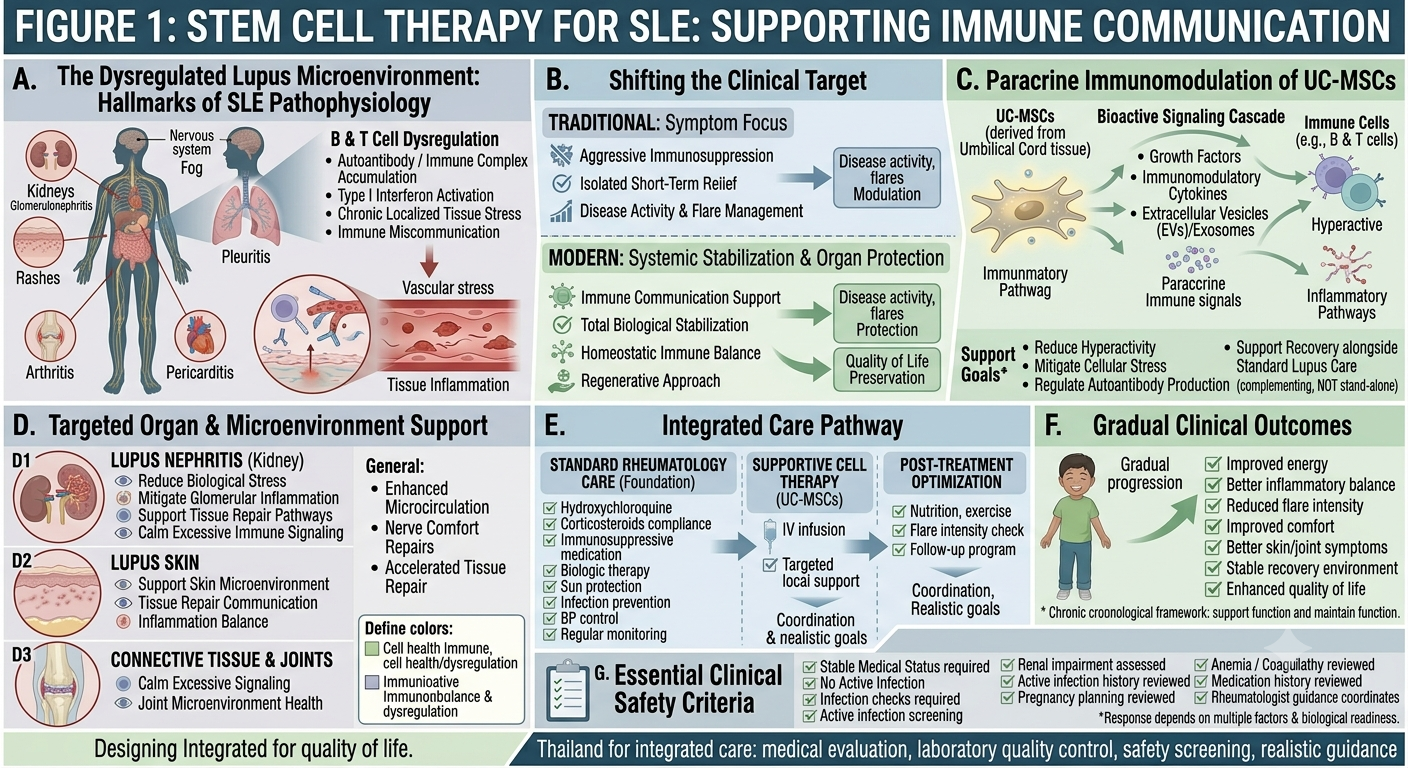 to steroids when required whilst preserving quality of life.
to steroids when required whilst preserving quality of life.
FIGURE 1: STEM CELL THERAPY FOR SLE: SUPPORTING IMMUNE COMMUNICATION
A New Way to Explain Stem Cell Therapy in SLE
One original and contemporary angle by which MSC stem cell therapy for SLE might be addressed is that of immune communication support.
Different research works are being conducted regarding mesenchymal stem cells or MSC stem cell therapy as they may have the ability to release bioactive signals which interact with immune cells, various inflammatory pathways, tissue repair processes and intercellular communication. It is important in autoimmune disease because it means that the immune system isn’t just ‘strong’ or ’weak. It is misdirected.
Stem cell based therapies for SLE should not be framed as immune system shutdown. An alternate explanation is that MSC stem cell therapy may promote an environment less skewed toward immune dormancy within a subset of patients.
Potential supportive goals may include:
Supporting inflammation balance
Supporting immune regulation
Helping calm excessive immune signaling
Supporting tissue repair communication
Supporting vascular and organ microenvironment health
Helping reduce biological stress during chronic inflammation
Supporting recovery alongside standard lupus care
This makes stem cell therapy different from standard immunosuppressive medication. It is not used to replace medication, but may be discussed as a supportive strategy under medical supervision.
Why the Lupus Microenvironment Matters
SLE, however, does not act alone on the immune system. And it influences the tissue environment itself, where inflammation occurs. A case in point is lupus nephritis, which results from inflammation of the kidneys. Lupus skin is lupus in the skin. Inflammation of the connective tissues surrounding a joint may play a role in non-joint pain. Fatigue: is it driven by inflammation, sleep disruption, anemia or drugs effects too? Or the activity of systemic disease process itself.
This is where the lupus microenvironment notion becomes useful. The immune and tissue microenvironment varies by the organ affected. Tissues that are under continuous inflammation can get damaged, be more easily stressed and slower to repair.
As MSC stem cell therapy improved the function of immune balance and signaling for tissue repair, stem-cell therapy may be considered. But each patient must be assessed on a case-by-case basis, particularly in the event of renal impairment, active infection history and significant anaemia / coagulopathy/ pregnancy planning with intense/high dose immunosuppressive therapy.
Standard SLE Treatment Still Comes First
Families should understand this clearly: SLE needs proper rheumatology care. Standard treatment may include hydroxychloroquine, corticosteroids when needed, immunosuppressive medication, biologic therapy, kidney-directed treatment, sun protection, infection prevention, blood pressure control, and regular monitoring.
Stem cell therapy should never be used as a reason to stop lupus medication by yourself. Stopping medication suddenly may increase flare risk and may be dangerous, especially for patients with lupus nephritis or major organ involvement.
A responsible regenerative medicine program should work around the patient’s medical history, current medications, disease activity, blood tests, organ involvement, and rheumatologist guidance.
What Families May Notice After Supportive Therapy
Possible supportive outcomes may include improved energy, better inflammatory balance, reduced flare intensity in selected patients, improved comfort, better skin or joint symptoms, improved recovery environment, or improved quality of life.
However, results vary widely. SLE is a complex disease. Response may depend on disease severity, kidney involvement, autoantibody profile, inflammation level, medication use, infection risk, stress, sleep, nutrition, and overall immune status.
The goal should be realistic: support the immune environment, reduce biological stress, and help the patient maintain function and quality of life alongside standard care.
Why Thailand for SLE Regenerative Medicine?
Thailand is increasingly known for regenerative medicine, wellness care, chronic disease support, and international patient services. Patients considering stem cell therapy for SLE in Thailand often look for an integrated approach that includes doctor evaluation, laboratory quality control, safety screening, and follow-up planning.
Before treatment, a responsible clinic should review blood count, kidney function, urine protein, inflammation markers, liver function, autoimmune profile, medication history, infection screening, pregnancy status if relevant, and disease activity.
Important Safety Note
Stem cell therapy for SLE remains an evolving and investigational area. It should not be marketed as a guaranteed cure, immune reset, or replacement for rheumatology care.
Patients with active infection, severe organ flare, unstable kidney disease, uncontrolled clotting problems, cancer history, pregnancy, or complex medication use require careful specialist review before any regenerative treatment is considered.
A trustworthy program should focus on patient selection, realistic goals, cell quality, medical supervision, safety monitoring, and coordination with standard lupus care.
Conclusion
Stem cell therapy for SLE in Thailand can be offered as a type of supportive regenerative medicine option to select patients with responsible explanation.
The single most original aspect of this approach is NOT to “reduce inflammation.” It has to do with facilitating immune signalling, balancing inflammation and promoting tissue repair signal transduction within the lupus microenvironment.
For the families, it’s not pursuing a miracle. The intent is to modulate the patient in a safe sense, safeguarding organs and flair burden when possible while improving health-related quality of life through an integrated approach directed by medical professionals balancing both regenerative medicine with traditional rheumatologic therapies.