

Introduction to the Devastating Impact of Motor Neuron Degeneration
Amyotrophic lateral sclerosis (ALS) is an incredibly damaging illness for patients and their families. This terminal illness attacks and degenerates the motor neurons of the cerebral cortex and spinal cord, leading to muscle atrophy and paralysis. Patients lose the ability to perform basic functions such as walking, talking, and even breathing, resulting in a dramatic decline in their quality of life over a long and agonizing process for both the patients and their loved ones. After the first appearance of symptoms, patients are expected to survive, on average, 2-5 years. The progression of the disease is relentless and highlights the critical need for the invention of new therapeutic strategies to slow the destruction of the cells. Advanced therapeutic strategies are of the utmost importance to the medical community. The use of UC-MSCs presents a highly positive approach to the treatment of the pathological deficits. The field of Regenerative Medicine Thailand wishes to focus on this area of cellular biology to treat the neurodegeneration caused by ALS.
Intricate Pathophysiological Mechanisms of the Disease
To fully understand cellular degeneration in ALS, various pathological cascades must be understood to advance UC-MSCs within Regenerative Medicine Thailand. The degeneration of motor neurons is severely caused by the excitotoxicity of glutamate. The release of the glutamate as a neurotransmitter is, in some cases, hyperactive to the level of damaging the neuron by flooding it with calcium ions. The elevated levels of calcium, in addition to damaging mitochondria, also exacerbated the oxidative stress. It is common for ALS patients to have accumulation of abnormally aggregated proteins, especially the TDP-43 mutant protein. Misfolded proteins can be found in the cytoplasm where they disrupt transport and create a toxic environment, leading to neuroinflammation. Reactive local microglia will release inflammatory cytokines such as tumor necrosis factor alpha. This results in an inflammatory cascade which compounds the apoptosis of motor neurons. The excitotoxicity paired with extensive and aggressive neuroinflammatory attacks creates a cycle of damage and death of neurons. This destructiveness is so extensive that it limits the effectiveness of traditional therapeutics, thus forcing Regenerative Medicine Thailand to consider the use of UC-MSCs as a primary treatment for ALS.
Constraints of Conventional Treatment Modalities
Current ALS pharmaceutical treatment options remain limited to a handful of available agents. Riluzole is the first agent that reduces excitotoxicity induced by glutamate and helps preserve the remaining neurons. Edaravone is another agent that is a free radical scavenger and decreases the oxidative stress and burden to the central nervous system. Unfortunately, the clinical benefits of these agents is very poor. The survival of patients is prolonged by only a few months and strength of the skeletal muscle is not improved. Damaged neurons are still not healed and the paralysis is still not controlled. Patients are still burdened by the need for infusions on a daily basis and the agents cause adverse effects, such as stress to the liver and a burden to the gastrointestinal system. Traditional treatment gaps are very large and continue to fuel the need for an expansive UC-MSCs cellular repair within Regenerative Medicine Thailand in order to combat the effects of ALS.
Mechanistic Benefits of Cellular Interventions
Within the context of neurodegenerative diseases, such as ALS, the use of UC-MSCs will help further the clinical and therapeutic goals. These cells are derived from umbilical cords and contain specific properties that are highly beneficial to the treatment of ALS. UC-MSCs are known to possess a strong paracrine signaling system. They release brain-derived neurotrophic factor (BDNF) as well as glial cell line derived neurotrophic factor (GDNF). Both of these proteins help motor neurons and other tissues repair and survive. In addition to this, UC-MSCs have strong immunomodulatory effects. These cells shift the inflammatory microglial cells to a protective microglial cell phenotype. This change helps to clear the damaging inflammatory reaction around dying motor neurons. These cells use tunneling nanotubes to transport healthy mitochondria to other cells and restore their energy. Compared to other cell therapies, these mesenchymal cells do not pose ethical problems and have great potential to grow. The broad spectrum of pathways these UC-MSCs address makes them the best option for Regenerative Medicine Thailand.
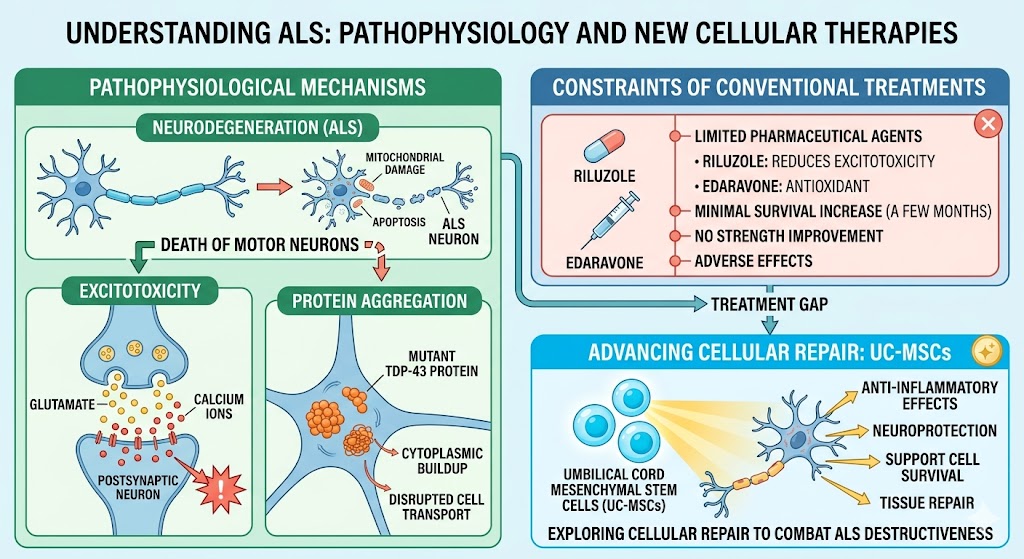
Figure 1: Mechanistic Benefits of Cellular Interventions in ALS
The Application of Cellular Therapies in Southeast Asia
Cellular therapies require an advanced healthcare system to support them, and Thailand is home to some of the best biotechnology services. Regenerative Medicine Thailand is supported by governmental and private investments in laboratory services. Thai scientists have a reputation for a high level of precision when isolating stem cells. When coupled with the accessibility to western healthcare systems, the trends show that Thai clinics may expedite localized clinical trials for treating ALS using UC-MSCs. There is a strong emphasis on establishing neurorestorative therapies in Thailand. The scientific partnerships that exist help to sustain translational discoveries. All factors support the development of both ALS therapies and UC-MSCs in Regenerative Medicine Thailand.
General Outlook of Current Therapies for ALS
The aim for therapies to combat ALS must consist of more than the management of cellular symptoms and strive for cellular restoration. Neuroinflammation co-morbid with excitotoxicity presents complexity that requires a poly-pharmaceutical approach. UC-MSCs provide an opportunity to achieve this by adjusting immune response and providing neurotrophic factors. Current medicinal therapies are largely palliative in nature as they slow an inevitable decline, whereas cellular therapies may offer genuine prospects for the repair of injured structures and restoration of lost functions. Developments in Regenerative Medicine Thailand are pioneering the establishment of these sophisticated ALS therapies using UC-MSCs. Integration of high-order cellular sciences in specialized clinical settings will provide a clear trajectory in addressing these severely impairing conditions. Promising outcomes are possible for actively treating terminal motor neuron diseases.