

Most patients who inquire me the most about stem cell therapy Thailand, they ask questions like; what if we inject? You are asked how many cells they will get, where the cells are delivered and when improvement may be seen.
These are important questions
But they’re not the whole story, though The injection is just one piece of the therapeutic puzzle when it comes to regenerative medicine. And of course, it also depends on what biological environmental those cells are hearing. Outcome is influenced by age, disease duration, inflammatory burden, glycemic control, lipid metabolism and vascular health as well as sleep quality or rehabilitation whereupon also the expectation of patients matters.
So, this is why I often say to patients that stem cell therapy does not just consist of passing cells into the organism. This is whether or not the body was biologically ready.
Stem cells operate within the host microenvironment
The studies of UC-MSCs focus more on the role of paracrine signaling rather than direct differentiation into tissue cells, and thus are classified as a type of MSC stem cell. They can, for example, secrete growth factors and cytokines in addition to extracellular vesicles (EVs) carrying proteins or non-coding RNAs that may act on immune cells as well as both endothelial and resident tissue cells.
In the academic sense, this is termed paracrine signalling and microenvironmental modulation.
Alternatively, in the most simple terms – stem cells might provide biological messages to classes of agents that regulate inflammation homeostasis and balance or influence immune modulation (as mentioned above), vascular signalling pathways involved with these processes and tissue repair signaling. But those signals do not work independently. Changing and responding to the existing internal state of a patient.
This healthiest of an internal environment may permit better interpretation by the regenerative signals. Disease environments that are highly inflamed/ metabolically unstable, or have reached a more structurally advanced stage may respond less unpredictably.
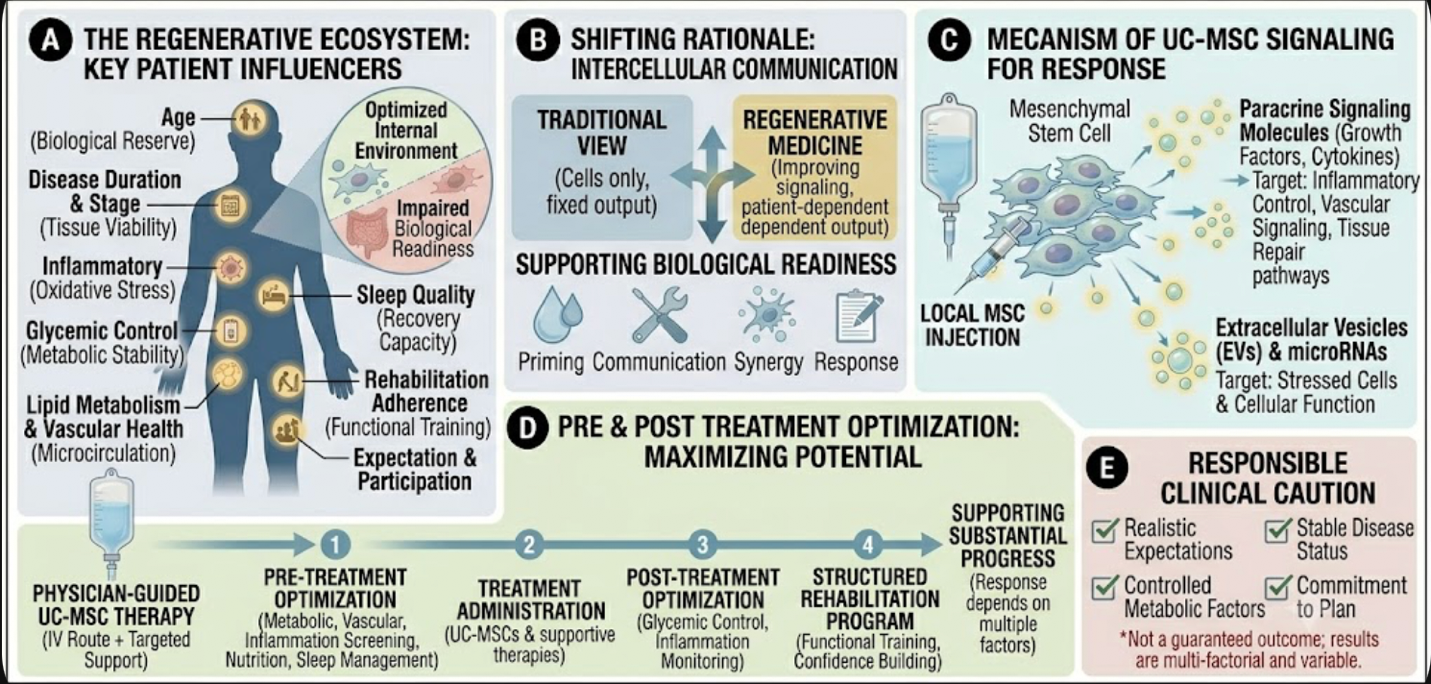
Figure 1: (A) The patient’s internal host microenvironment, mapping key biological influencers: physiological reserve, remaining tissue viability, systemic inflammatory burden, glycemic/lipid stability, sleep-driven recovery, and rehabilitation compliance. (B) Shifting the clinical rationale from a fixed-output therapeutic view to an interactive signaling framework that relies on systemic readiness. (C) Paracrine signaling cascade of Umbilical Cord-derived Mesenchymal Stem Cells (UC-MSCs) secreting growth factors, cytokines, and non-coding RNA-loaded extracellular vesicles (EVs). (D) Chronological timeline for pre- and post-treatment optimization protocols to maximize signaling interpretation and clinical progress. (E) Standard clinical criteria for safe patient selection and the mitigation of unrealistic patient expectations.
Age and Biological Reserve
It matters as much for the years lived than that answer. Biological reserve however is much more relevant.
Two patients the same age might be wildly different in their health profiles. One might have great circulation, stable blood sugar levels, strong muscle mass,, solid sleep habits and a regular routine of exercise. One may be suffering from chronic inflammation along with poor metabolic control, vascular disease and little physical activity.
The second patient might have a worse repairing capability, although the treatment protocol is similar.
Not that patients older than 70 can not get stem cell therapy. It involves realistically acknowledging what can be achieved as the goal of treatment. Hence for some patients, it may not be complete structural reversal that is the goal but improved comfort and mobility or less inflammatory burden with slowed functional decline.
Disease Stage and Tissue Viability
Stage of the disease is one of the strongest predictors for response.
A patient with mild arthritis and well-preserved joint space may behave differently than a more severely compromised, bony on bone degenerative case. A patient who has some early disc degeneration still might be one in whom much function of the care tissue is retrievable compared to a more advanced collapse, severe stenosis or chronic nerve injury.
Although stem cell therapy may provide supportive treatment to the regenerative microenvironment, it does not always overcome irreversible structural damage. Imaging, laboratory evaluation and symptomatology history and physician assessment are thus mandates before making a treatment plan as to the reason for heart failure.
Now you are trained in the fact that it is not only, WHAT disease do you have?
The more pressing question is, “How much function of that tissue remains viable?
Glycemic Control and Metabolic Stability
Another big one is blood sugar. Indeed, chronic hyperglycemia may adversely affect the endothelium function and increase oxidative stress status leading to an impaired wound healing capacity and reduced tissue repair ability (Sahu et al., 2021; Sosa-Henríquez et al., 2018). Regenerative response may be less predictable in patients with diabetes or insulin resistance, particularly when metabolic control is inadequate.
In diabetic patients, this would not be an exclusion from treatment. That simply means that what glycogenic stability should be included in the framework preparation process. Review of HbA1c, fasting glucose, renal function status and wound assessment (stability/intended treatment stage), circulation perioperatively/infection risk should also be conducted carefully.
A regenerative program not a nice-to-have, but integrated into metabolic medicine rather than separate from it — this is the solution that works best.
Lipids, Vascular Health, and Circulation
Cholesterol, triglycerides and the state of vascular health — patients drastically underestimate their contribution to successful regenerative outcomes.
The vascular system (blood and lymphatic vessels) supplies oxygen, nutrients, immune cells and repair signals to tissues. Recovery may be delayed when endothe-lial dysfunction, lipid accumulation within the vessel wall and inflammation are associated with poor microcirculation.
This is of particular relevance to those patients with diabetes, cardiovascular risk, chronic wounds, erectile dysfunction and/or kidney or degenerative joint disease. In such cases, it may be the support of vascular health that is equally as important (perhaps more so) than the stem cell protocol itself!
It may be a helpful signal or it can also cause chronic barrier in the body: Inflammation
Inflammation is not always bad.
Acute inflammation is a response of the body to an injury.
But the challenge comes when chronic inflammation turns into a biological barrier to healing.
When inflammatory cytokines are present and oxidative stress is ongoing for long durations of time, the tissue environment may become less regenerative and more degenerative in nature owing to immune dysregulation. This may impair the action of any regenerative intervention.
Thus, some patients could greatly benefit from pre-treatment optimization such as nutrition, sleep improvement, infection control, metabolic management and anti-inflammatory lifestyle support coupled with physician-guided adjunctive therapies as appropriate.
Sleep, Rehabilitation, and Daily Behavior
Sleep is a biological necessity and an oft disregarded need. Impaired sleep also interferes with inflammation, glucose regulation, pain sensitivity and hormonal balance as well as reducing recovery capacity.
Rehabilitation is equally important. Biology may support stem cell therapy, but rehabilitation translates biological support into functional improvement. Structured movement training aids in restoring strength, coordination, balance and confidence from joint, spine neurological and post-injury conditions.
Patients are more likely to have a better functional pathway with active participation in rehabilitation.
Final Perspective
Stem cell therapy response depends on much more than just the injection. It is affected by the biological reserve of the specific patient (biological age), stage of illness, metabolic state, vascular status at baseline, buried inflammatory burden, sleep quality and quantity during hospitalization and post-operative rehabilitation adherence coupled with reasonable expectations.
If you are researching stem cell therapy in Thailand, the question is not only “How many cells am I getting?”
The next question is more clinically relevant:
What do we optimize from a pre & post treatment standpoint to maximize the potential for substantial progress and, am I primed to respond or will my body simply ignore any regenerative signaling?