

The clinical progression of translational regenerative medicine is increasingly moving away from monotherapy models. For years, the primary objective of cellular transplantation centered on identifying a single, optimal cell source such as bone marrow, adipose tissue, or neonatal membranes to address systemic degradation or localized tissue trauma. While these single-source applications have delivered notable therapeutic milestones, they frequently hit a biological wall when tasked with resolving complex, multi-system disorders that require simultaneous structural scaffolding and intense immunomodulatory signaling.
To cross this therapeutic threshold, advanced protocols utilize a dual-source cellular matrix pairing Umbilical Cord Mesenchymal Stem Cells (UC-MSCs) with Placenta-Derived Stem Cells. This combination does not merely increase total cell volume; instead, it establishes a distinct biological synergy. By merging the highly active, young proliferative signaling of UC-MSC stem cell therapy with the rich, extracellular matrix (ECM) structural components native to placental tissue, clinicians can trigger an enhanced regenerative cascade. This combined approach optimizes tissue integration, accelerates wound healing, and resolves complex tissue defects with a level of efficacy that single-source therapies cannot achieve.
1. Ontogenetic Foundations: Decoding the Dual-Source Architecture
The scientific rationale for combining these two distinct neonatal tissues rests on their shared origin and complementary developmental functions. Both the umbilical cord and the placenta are temporary embryonic organs formed during gestation to nourish, protect, and build human life. However, their internal cellular niches prioritize different biological mechanisms.
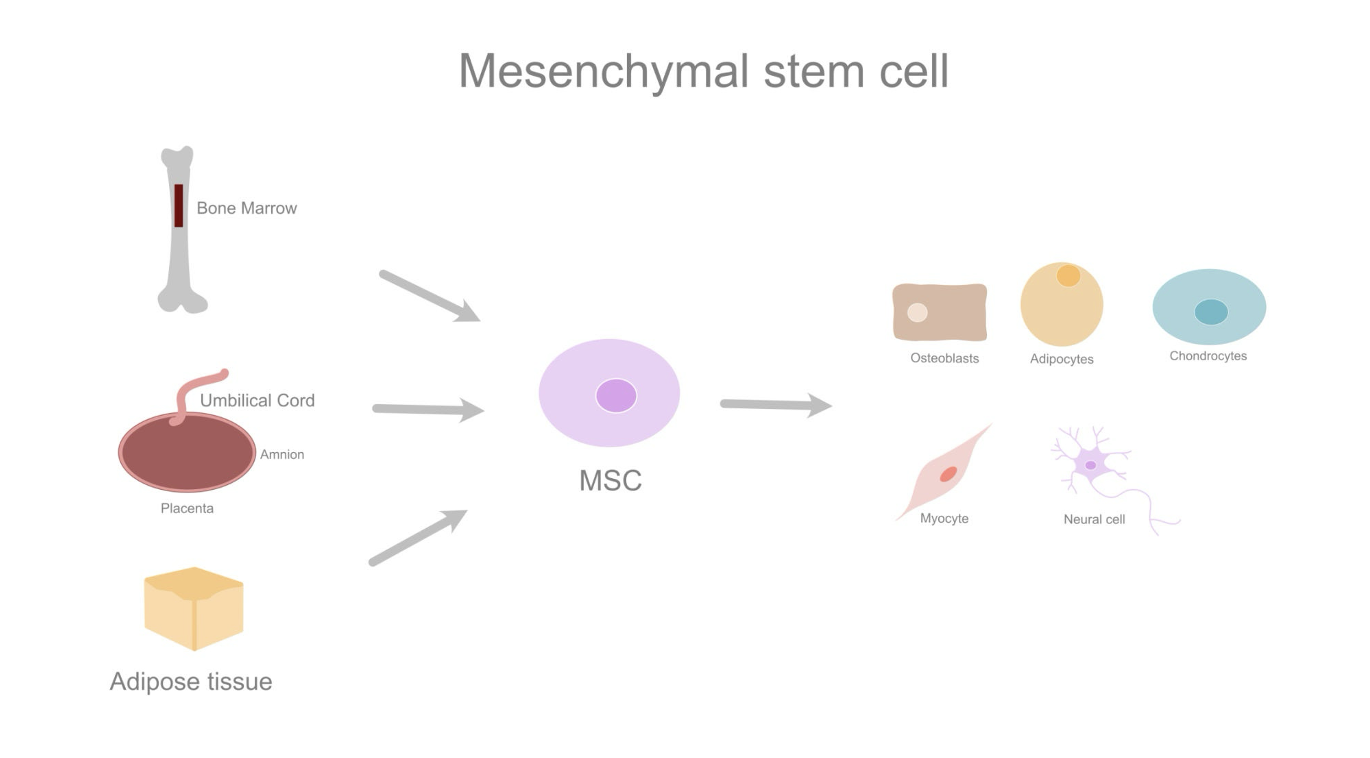
Figure 1: Neonatal and adult sources of multipotent Mesenchymal Stem Cells (MSCs).
As illustrated in the anatomical lineage diagram above, Mesenchymal Stem Cells (MSCs) isolated from neonatal structures represent a distinct mid-point between pluripotent embryonic cells and restricted adult progenitor cells. Sourcing cells from both the umbilical cord and the placenta allows clinicians to leverage two highly specialized cellular profiles:
The Proliferative Vitality of UC-MSC Stem Cell Therapy
Isolated primarily from the specialized gelatinous connective tissue known as Wharton’s Jelly, UC-MSC stem cell therapy are considered “day-zero” cells. Because they are collected at the exact second of birth, they are completely uncompromised by the environmental stress, telomere shortening, or metabolic waste accumulation that limits the potency of adult autologous cell sources. UC-MSC stem cell therapy demonstrate rapid replication kinetics, excellent chromosomal stability, and an extraordinary capacity to secrete anti-inflammatory cytokines.
The Structural Support of Placenta-Derived Cells
While UC-MSC stem cell therapy excel at active, long-range chemical signaling, stem cells isolated from the chorionic villi and amniotic membranes of the placenta are biologically engineered for structural protection and matrix deposition. The placental niche contains a high density of cells that specialize in manufacturing key structural components, remodeling damaged tissue boundaries, and secreting specialized matrix metalloproteinases (MMPs) that dissolve old, rigid scar tissue to make way for healthy tissue integration.
2. Paracrine and Scaffolding Dynamics: Mechanisms of Biological Cooperation
When UC-MSC stem cell therapy and Placenta-Derived stem cells are co-administered, they do not act as isolated units. Instead, they form a cooperative biological network where the actions of one cell population enhance the therapeutic survival and performance of the other.
The Paracrine Cascade
Mesenchymal stem cells do not repair damaged tissues primarily by morphing directly into new host cells. Instead, their chief therapeutic mechanism is paracrine communication, the continuous synthesis and secretion of growth factors, active cytokines, and extracellular vesicles called exosomes that reprogram the surrounding tissue environment.
In a dual-source protocol, this paracrine output expands into a multi-layered molecular cascade. UC-MSC stem cell therapy release high concentrations of Brain-Derived Neurotrophic Factor (BDNF) and Transforming Growth Factor-beta (TGF-), which work systematically to cool down tissue-damaging inflammation and protect weak host cells from premature cell death.
Simultaneously, the Placenta-Derived cell population acts directly upon the local tissue architecture. As detailed in the cellular function diagram below, these cells function like advanced architectural factories, producing a dense matrix of structural support factors.
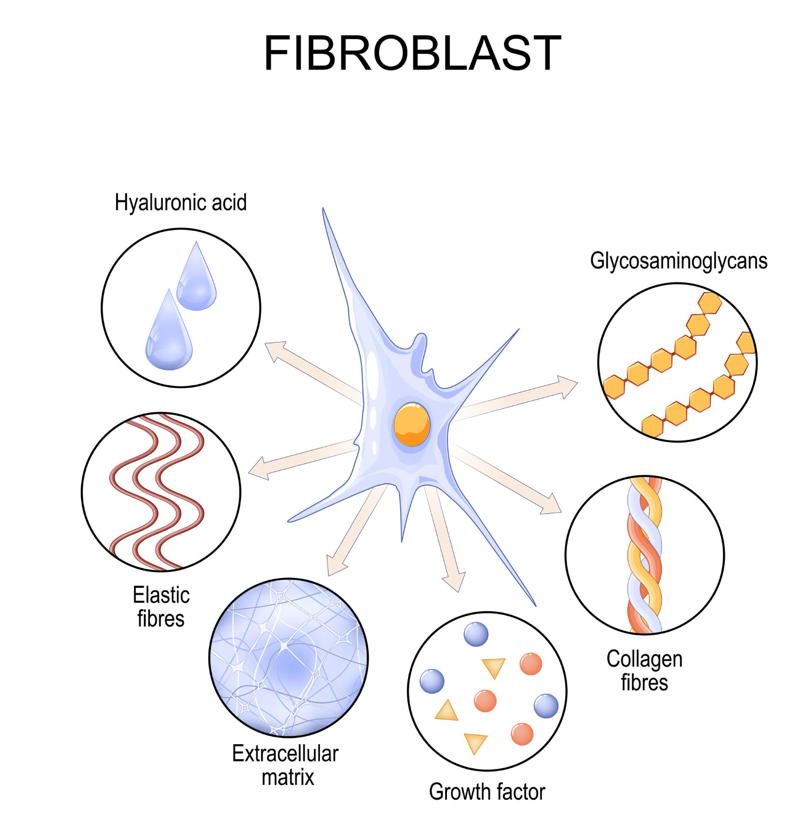
Figure 2: Cellular synthesis and deposition of extracellular matrix components.
The placental cells deposit a rich network of collagen fibers, elastic fibers, and glycosaminoglycans directly into the wound bed. This immediate structural scaffolding acts like a physical trellis, stabilizing the damaged area and providing an optimal physical surface where the highly mobile UC-MSC stem cell therapy can dock, survive, and continuously broadcast their anti-inflammatory signaling packages.
Furthermore, the simultaneous release of hyaluronic acid from this dual matrix keeps the local fluid environment highly hydrated, reducing mechanical stress on struggling host tissues and accelerating the migration of resident repair cells into the injury core.
3. The Synergy Matrix: Quantifying Dual-Source Interventions
To understand how this dual-source cellular model operates across complex clinical indications, it helps to analyze the specific biological targets and the corresponding cooperative mechanisms triggered by this cellular pairing:
| Therapeutic Target | Single-Source Limitation | Dual-Source Synergistic Intervention | Clinical Relevance |
| Vascular Network Repair (Angiogenesis) | Single cell lines produce limited variations of vascular signals, sometimes leading to fragile micro-vessel growth. | UC-MSCs release high volumes of VEGF, while Placenta cells provide Angiopoietin-1 and basic Fibroblast Growth Factor (bFGF). Together, they build stable, mature capillary tubes. | Critical for resolving ischemic tissues, advanced diabetic foot ulcers, and poorly oxygenated organ matrices. |
| Severe Tissue Fibrosis (Scarring) | Suppressing inflammation alone cannot dissolve dense, pre-existing structural scar barriers. | UC-MSCs halt the activation of scar-forming myofibroblasts, while Placenta-derived factors secrete precise MMPs to break down rigid collagen knots. | Essential for restoring flexibility to arthritic joints and preventing permanent strictures in Crohn’s Disease. |
| Hyper-Reactive Autoimmunity | High systemic inflammation can overwhelm single cell injections, leading to lower cell survival rates. | Placenta cells establish an immediate, localized immunoprivileged shield, allowing the UC-MSCs to safely re-educate overactive white blood cells. | Optimizes outcomes for aggressive conditions like Lupus (SLE), Rheumatoid Arthritis, and advanced neuroinflammation. |
Conclusion: Advancing the Standards of Translational Medicine
Ultimately, the integration of Umbilical Cord Mesenchymal Stem Cells and Placenta-Derived cellular matrices represents a major step forward for translational medicine. By moving past the constraints of single-source therapies, this cooperative model mimics nature’s own embryonic development systems combining intense anti-inflammatory communication with robust structural scaffolding.
Choosing a clinical framework that prioritizes fresh, dual-source neonatal cultures processed under strict international laboratory benchmarks ensures that your investment in regenerative medicine delivers maximum safety, optimal tissue integration, and genuine, life-changing functional recovery.