

Management of autoimmune endocrine failure, in particular Type 1 Diabetes (T1D) is potentially one of the most severe pathophysiological challenges presented to modern metabolic medicine. Type 1 Diabetes is a condition associated with an autoimmune, T-cell mediated elimination of insulin-secreting beta cells in the pancreatic islets of Langerhans that results in instant, absolute dependence on exogenous insulin replacement for life. Standard medical care has used a purely defensive, palliative framework for decades. Continuous glucose monitoring systems (CGMs) availability, interconnected automated insulin pump networks and precise carbohydrate-to-insulin ratios used both as diagnostic and stabilization tools.
These classical external delivery matrices only substitute the lost hormone, they do not alter the auto-immune cascades that are cruising behind the curtain to destroy the organism. While the endocrine system can recover over time, administration of exogenous hormone does not fix the long-lasting auto-reactive cellular environment and will never stop long-term issue tissue decline like diabetic nephropathy, retinopathy, and fringe autonomic neuropathies.
To address these core biological failures, modern translational research leverages advanced protocols of stem cell therapy bangkok thailand to shift the metabolic care paradigm toward direct microenvironmental modification. By introducing high-potency, ethically isolated neonatal Umbilical Cord Mesenchymal Stem Cells (UC-MSCs), clinical platforms seek to reset the un-balanced immune system.
Administered through optimized, highly controlled systemic frameworks, these day-zero cell lines act as active mobile signaling hubs. They navigate toward inflamed pancreatic pathways, suppress hyper-reactive cytotoxic immune profiles, protect remaining islet configurations from premature programmed cell death (apoptosis), and promote a receptive physiological landscape for long-term Regenerative Wellness.
The Autoimmune Crisis: T-Cell Overactivation and Islet Degradation in Type 1 Diabetes
To understand why traditional treatments fall short and how advanced stem cell therapy bangkok thailand modifies clinical outcomes, the pathological lens must examine the precise neuro-immunological environments operating within the pancreatic tissue beds. In Type 1 Diabetes, the structural destruction of the endocrine infrastructure is driven by a profound breakdown in immune tolerance.
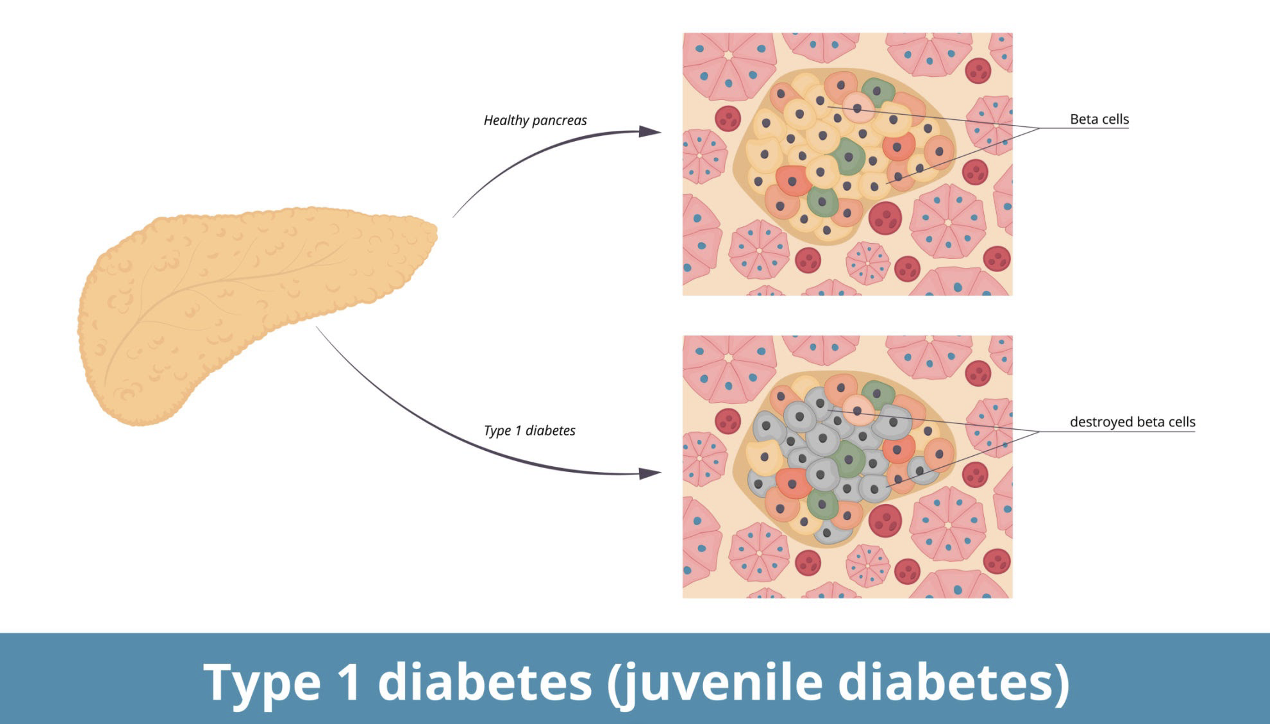
Figure 1: The autoimmune mechanism of pancreatic beta-cell destruction in Type 1 Diabetes.
The normal pancreas shown in the top half of this comparative tissue map (above) has a tightly regulated endocrine matrix composed of functional beta cells (-cells) that constantly sense circulating glucose and secrete just the right amount of insulin, a powerful regulatory hormone. This homeostatic state completely collapses in the onset of Type 1 Diabetes. Instead, the above mentioned specific native proteins expressed on a subset of beta-cells are recognized as non-self by the immune system, e.g. Glutamic Acid Decarboxylase (GAD65) or Insulinoma-Associated Protein 2 (IA-2).
This error promotes an exaggerated influx of cells due to activated antigen presenting cells that recruit hyper-activated T-cells and pro-inflammatory Th1/Th17 helper types directly into islet matrices.
This localized auto-reactive team floods the delicate endocrine microenvironment with high concentrations of destructive cytokines, primarily Interferon-gamma (IFN-), Interleukin-1β, and Tumor Necrosis Factor-alpha (TNF-). This chronic chemical exposure forces the resident beta cells into accelerated apoptosis, progressively reducing functional beta-cell mass until the body completely loses independent glycemic control.
Molecular Mechanisms of Rejuvenation: The Tri-Phasic MSC Secretome
Allogeneic Umbilical Cord Mesenchymal Stem Cells present a potent new biological therapy for Type 1 Diabetes because they avoid the biological barriers, environmental insults and cellular aging that impair adult self-derived (autologous) bone marrow or fat harvests. Obtained only through ethically restricted Wharton’s Jelly of healthy, full-term neonatal donor tissues, these cells possess extraordinary proliferative potential as well as longer telomere lengths. Completely immunoprivileged as they do not express HLA Class II surface antigens, these cells can be implanted without any human leukocyte antigen matching or need for long-term immunosuppression.
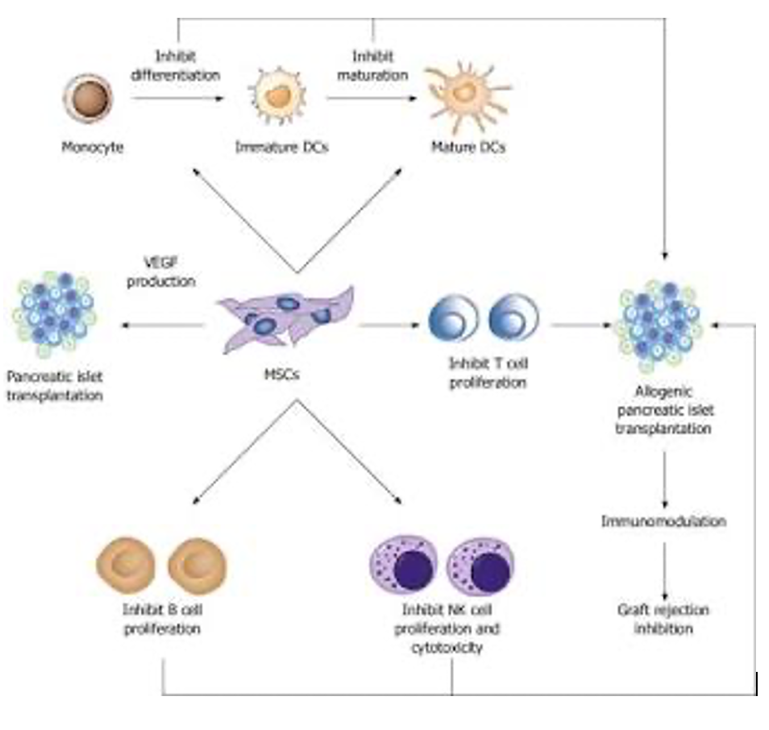
Figure 2: Mesenchymal stem cell signaling pathways for autoimmune suppression and islet matrix protection.
As detailed in the mechanism blueprint above, the therapeutic efficacy of deploying stem cell therapy bangkok thailand is driven entirely by paracrine signaling and secretome dynamics within the compromised metabolic axis. When introduced into a patient presenting with active Type 1 Diabetes, UC-MSC stem cell therapy bangkok thailand alter the degraded auto-immune microenvironment through a tri-phasic molecular cascade:
Macro-Immunomodulation and Regulatory T-Cell () Polarization
The primary therapeutic milestone achieved by UC-MSC stem cell therapy bangkok thailand is the systematic re-programming of the hyper-reactive cellular immune profile. As shown in the signaling pathway map, MSCs actively interact with multiple branches of the immune framework. They secrete powerful anti-inflammatory signaling molecules, including Indoleamine 2,3-dioxygenase (IDO), Transforming Growth Factor-beta (TGF-), and Prostaglandin E2 (PGE2).
This localized release directly suppresses the proliferation and cytotoxicity of auto-reactive T-cells and natural killer (NK) cells. Concurrently, it inhibits the maturation of dendritic cells, stopping the continuous presentation of self-antigens.
Most importantly, this paracrine payload drives the differentiation of naive T-cells into protective Regulatory T-cells ( cells). These units act as systemic immune stabilizers, migrating into the pancreatic islets to permanently turn off the auto-reactive fire, thereby protecting surviving beta-cell structures from ongoing autoimmune destruction.
Exosome-Mediated Beta-Cell Rescue and Mitochondrial Recovery
UC-MSC stem cell therapy bangkok thailand function as advanced mobile factories, discharging millions of microscopic, membrane-bound extracellular vesicles called exosomes into circulation. These vesicles traverse dense tissue boundaries to fuse with the plasma membranes of weak, struggling beta cells, delivering a highly concentrated payload of non-coding microRNAs (such as miR-21 and miR-146a) and vital bio-energetic proteins directly into the cytoplasm.
This cargo delivery restores healthy mitochondrial ATP energy production, downregulates the pro-apoptotic Bax pathways, and rescues surviving beta cells from cytokine-induced cell death, helping to preserve remaining independent insulin-secreting capacity in patients with Type 1 Diabetes.
Angiogenic Support and Microvascular Remodeling
To preserve the structural integrity of the islets, the surrounding vascular network must be actively protected. Stressed pancreatic beds experience severe microvascular narrowing and localized tissue ischemia due to chronic auto-immune inflammation. UC-MSC stem cell therapy bangkok thailand combat this physical restriction by producing high volumes of pro-angiogenic factors, primarily Vascular Endothelial Growth Factor (VEGF) and basic Fibroblast Growth Factor (bFGF).
These signaling proteins interact with nearby endothelial cells, commanding them to sprout a dense network of fresh micro-capillaries directly into the islet margins. Restoring local blood flow ensures an immediate, abundant supply of oxygen and systemic nutrients, stabilizing the endocrine microenvironment.
Beyond Cryopreservation: Preserving Day-Zero Potency in Bangkok
In the case of complex conditions like Type 1 Diabetes, the clinical success of stem cell therapy bangkok thailand is governed by nothing less than cellular viability at the point-of-care. Although there are practical reasons for cryopreservation, such as scaling up cell distribution across global logistics networks, cryopreservation relies on subjecting cellular suspensions to deep-freezing protocols using chemical cryoprotectants (such as Dimethyl Sulfoxide (DMSO)this methodology exerts significant thermodynamic stress on the delicate plasma membrane. Bedside thawing cascades often trigger expedited cell lysis and down-regulation of the expression of the homing receptors required for specific transendothelial migration in the context of degraded pancreatic tissue beds.
In order to address this logistical bottleneck, state-of-the-art biomedical facilities administering theraputic stem cell therapy bangkok thailand utilise a continuous closed-system culture system which runs via stringent international Good Manufacturing Practises (GMP). Technicians extend neonatal umbilical cord lineages locally by performing aseptic processing in Class-A laminar flow cleanrooms backed up by positive-pressure HEPA filtration. This close proximity to the clinical environment negates the need for cryoprotective vitrification.
The processed SACG adhere in a temperature-controlled, nutrient-rich transport matrix right until the moment of clinical application. Viability scores reported exceeding 95% verified by automated cytometry and fluorescence-based live/dead assays Thus, it is this fusion of architectural and logistical forces that guarantees a coactive secretome cargo delivery to the recipient, which consequently benefits from maximized paracrine signaling efficiency, and prefers tissue remodeling sculpted under structural constraints within inflamed microenvironments.
Real-World Expectations: Defining Objective Clinical Indicators
When discussing advanced cellular therapies for Type 1 Diabetes, maintaining absolute honesty, transparency, and a grounded perspective is essential. Stem cell therapy bangkok thailand is not a magical overnight cure that allows a patient to instantly disregard core medical guidelines, continuous glucose tracking, or healthy dietary structures. Instead, it serves as a powerful biological accelerant that works hand-in-hand with clinical management to alter the disease’s path.
Patients responding well to advanced UC-MSC metabolic protocols typically observe gradual, progressive health improvements over a window of two to six months:
Stabilized C-Peptide Secretion: A measurable preservation or steady increase in baseline and stimulated C-peptide metrics. Because C-peptide is manufactured and released in a 1-to-1 ratio alongside endogenous insulin, its stabilization provides definitive biological proof of successful beta-cell rescue.
Lowered Daily Insulin Demands: A systematic reduction in total daily exogenous insulin units (both basal and bolus requirements) while maintaining stable, target-range glycemic profiles.
Optimized Time-in-Range (TIR): A significant reduction in blood glucose variability, resulting in fewer dangerous nighttime hypoglycemic dips and less extreme post-meal glycemic spikes.
Mitigation of Vascular Complications: Measurable improvements in peripheral nerve conduction, accelerated healing of minor skin tears, and a systemic down-regulation of circulating vascular inflammatory markers.
Clinical Integration Blueprints: The Somatic Restoration Continuum
Stepping into an advanced clinical pipeline for stem cell therapy bangkok thailand operates via a meticulously timed, objective medical execution strategy focused entirely on patient safety and structural tissue matrix optimization.
1.Pre-Therapeutic Biomarker Prototyping and Patient Stratification
Phase I
The clinical journey initiates with a deep molecular evaluation of the patient’s complete diagnostic profile, current fasting insulin lines, circulating GAD65/IA-2 auto-antibody titers, baseline C-peptide metrics, and targeted metabolic blood panels to confirm absolute biochemical suitability for treating Type 1 Diabetes.
2.GMP-Compliant Bio-Manufacturing and Sterility Assurance
Phase II
Upon formal diagnostic verification, a partnered PIC/S GMP-certified laboratory executes the controlled expansion of fresh, non-cryopreserved allogeneic cell lines. The customized culture undergoes automated cytometric assays to guarantee exceptional cellular viability scores and verified sterile release parameters prior to formulation.
3.Precision Chrono-Pharmacological Deployment and Monitored Transplantation
Phase III
The formulated concentration of high-potency, day-zero cells is delivered within an advanced medical environment. The cell matrix is steadily administered via systemic intravenous (IV) infusions under continuous multi-parametric medical tracking, ensuring zero recovery downtime and maximum cell yield.
4.Post-Transplantation Secretome Potentiation and Homeostatic Stabilization
Phase IV
Following clinical delivery, specialized medical teams deploy comprehensive, personalized recovery frameworks, incorporating targeted micronutrient strategies, anti-inflammatory dietary pacing, and metabolic co-factors engineered to sustain a highly receptive internal environment and maximize long-term beta-cell survival in Type 1 Diabetes.
Conclusion: Reclaiming Control of Your Metabolic Future
Type 1 Diabetes is marked by relentless, progressive auto-immune phenomena resulting in the destruction of insulin-producing beta-cells, However patients and families need not be forever trapped in an exclusively reactive loop of symptomatic management through transient civil service of exogenous insulin whilst their existing volume responsible for makeshift reward assumes full structural atrophy. It is still clearer that simple superficial hormone replacement which treats the epidermis of a profound cell and immunobiological collapse merely disguises tissue decline while leaving the real metabolic catastrophe unaddressed.
By opting for sophisticated, ATMP-regulated stem cell therapy bangkok thailand you deliver your system the extremely powerful, youth-derived assets it must calm chronic islet irritation and sustain protecting cell polarization shielding enduring pancreatic beta cells from the in. It is a bold, forward-thinking movement toward postponing progressive vascular complications and strengthening endogenous glycemic control that are profoundly impactful by building an even stronger capability for your metabolic independence under the rigid oversight of Thailand’s PIC/S GMP guidelines governing all regenerative medicine.