

Parkinson’s disease is often introduced as a disorder of dopamine loss, but that explanation is no longer enough. The loss of dopaminergic neurons in the substantia nigra remains central to Parkinson’s disease, yet the condition is now understood as a multi-system neurodegenerative process involving alpha-synuclein aggregation, mitochondrial dysfunction, oxidative stress, impaired autophagy, neuroinflammation, synaptic instability, and immune-neural communication.
This is why a serious article about stem cell therapy bangkok thailand for Parkinson’s disease should not begin with a generic explanation of what stem cell therapy bangkok thailand are. That content has already been repeated across thousands of websites. A more useful discussion begins at the disease environment itself: why neurons become vulnerable, why inflammation persists, why mitochondrial energy failure matters, and why secretome-based signaling is being studied as a possible supportive mechanism.
For patients researching stem cell therapy bangkok thailand, the most important point is clarity. Stem cell-based approaches should not be presented as a cure, a replacement for standard neurological treatment, or a guaranteed way to reverse Parkinson’s disease. The National Institute of Neurological Disorders and Stroke states that Parkinson’s disease currently has no cure, although medicines and surgery may help improve symptoms and movement.
A stronger and more medically responsible question is not “Can stem cells replace dopamine?” The better question is: Can regenerative cell signaling influence the biological stress loops that contribute to Parkinson’s disease progression?
Parkinson’s Disease as a Multi-System Neurodegenerative Stress Loop
Parkinson’s disease is traditionally linked with dopamine neuron loss and alpha-synuclein accumulation. However, current research increasingly describes Parkinson’s disease as a complex disorder involving multiple interacting pathways rather than a single isolated dopamine problem. Aggregated alpha-synuclein may contribute to neuroinflammation, mitochondrial dysfunction, impaired autophagy, endoplasmic reticulum stress, reactive oxygen species production, and synaptic disruption.
These pathways often reinforce each other. Alpha-synuclein misfolding may increase cellular stress. Cellular stress may activate microglia. Activated microglia may release inflammatory cytokines and oxidative mediators. Inflammation may worsen mitochondrial injury. Mitochondrial dysfunction may increase oxidative stress. Oxidative stress may further impair protein clearance.
This self-reinforcing cycle explains why regenerative medicine content should move away from simple claims such as “repairing damaged neurons.” The more intelligent framework is mechanism-based: reducing hostile inflammatory tone, supporting mitochondrial resilience, improving extracellular communication, and protecting surviving neural networks from ongoing biological stress.
Mechanism 1: Alpha-Synuclein Stress and Protein-Clearance Failure
Alpha-synuclein is a presynaptic protein that can misfold and aggregate in Parkinson’s disease. These abnormal aggregates may interfere with synaptic communication, mitochondrial function, lysosomal activity, and cellular survival pathways. Research reviews describe alpha-synuclein pathology as a central driver of toxic cascades in Parkinson’s disease, especially when protein clearance systems fail.
The brain normally relies on autophagy, mitophagy, lysosomal degradation, and ubiquitin-proteasome pathways to manage damaged proteins and organelles. When these systems become impaired, abnormal protein accumulation can increase. A 2025 review describes autophagy as essential for neuronal homeostasis because it helps degrade and recycle damaged proteins and organelles.
stem cell therapy bangkok thailand for Parkinson’s disease should not be described as directly clearing alpha-synuclein from the human brain. That would be too strong. A more accurate explanation is that secretome-based signaling may support a less inflammatory and less oxidatively stressed microenvironment, which may indirectly influence the cellular systems involved in protein homeostasis.
This wording matters. It creates a scientifically mature article rather than a promotional treatment page.
Mechanism 2: Microglial Activation and Neuroinflammatory Pressure
Microglia are resident immune cells in the central nervous system. In a healthy brain, they participate in surveillance, debris clearance, synaptic remodeling, and injury response. In Parkinson’s disease, microglia may become chronically activated and contribute to a persistent inflammatory environment.
This inflammatory state can expose vulnerable neurons to cytokines, reactive oxygen species, nitric oxide signaling, and other stress mediators. Neuroinflammation is especially important because it does not only respond to damage; it may also amplify damage when it remains active for too long.
The proposed relevance of MSC-based secretome signaling is not broad immune suppression. The more precise mechanism is immune rebalancing. Secreted mediators and extracellular vesicle cargo may influence microglial behavior, cytokine networks, oxidative stress responses, and repair-associated signaling.
For stem cell therapy bangkok thailand content, this is a stronger angle than simply saying “stem cell therapy bangkok thailand reduce inflammation.” The article should explain which inflammatory system matters, why chronic activation is harmful, and how regulatory signaling may be biologically relevant.
Mechanism 3: Mitochondrial Dysfunction and Energy Collapse
Dopaminergic neurons are metabolically demanding cells. They maintain long axonal projections, continuous neurotransmitter cycling, calcium handling, synaptic signaling, and cellular repair. Because of this high energy demand, mitochondrial dysfunction is one of the most important mechanisms in Parkinson’s disease biology.
When mitochondria fail, ATP production may decline and oxidative stress may increase. This can worsen synaptic instability, protein misfolding, calcium imbalance, and neuronal vulnerability. A 2025 review on MSC stem cell therapy bangkok thailand and neurodegenerative diseases highlights mitochondrial damage as an important translational target while also emphasizing the limitations and challenges of MSC-based strategies.
MSC-derived signals may be studied for their relationship with antioxidant pathways, mitochondrial stress responses, extracellular vesicle cargo, and cell-survival communication. Some experimental research also explores mitochondrial transfer between cells, including through tunneling nanotubes, but this should be presented as a research mechanism rather than a guaranteed clinical effect.
A responsible article should say: mitochondrial support is a proposed biological pathway, not proof that stem cell therapy bangkok thailand can reverse Parkinson’s disease.
Mechanism 4: Extracellular Vesicle Signaling and Secretome Communication
Extracellular vesicles are small membrane-bound signaling particles released by cells. They may carry proteins, lipids, messenger RNA, microRNA, and other regulatory molecules. In MSC research, extracellular vesicles are important because many of the proposed effects of MSC stem cell therapy bangkok thailand may be mediated through secreted molecular communication rather than permanent engraftment.
This is one of the most useful mechanisms to include in a modern article on stem cell therapy bangkok thailand for Parkinson’s disease. It moves the discussion away from the outdated idea that stem cell therapy bangkok thailand simply become new brain cells. Instead, it explains that cell-to-cell signaling may be one of the most important areas of investigation.
A 2025 systematic review described MSC-derived extracellular vesicle therapy in Parkinson’s disease as a developing research area and reported gradual improvements in preclinical models, while still requiring further validation before it can be treated as established clinical proof.
Potential extracellular vesicle-related mechanisms include:
Modulation of microglial activation
Delivery of anti-inflammatory microRNAs
Support for antioxidant signaling
Regulation of apoptosis-related pathways
Interaction with mitochondrial stress responses
Trophic communication with stressed neural networks
These pathways are scientifically interesting, but they should be framed as investigational. Mechanism does not automatically equal clinical efficacy.
Mechanism 5: Dopaminergic Circuit Support Without Claiming Cell Replacement
Many Parkinson’s disease articles focus too heavily on dopamine neuron replacement. That approach can confuse patients because different types of stem cell research are being mixed together.
Dopamine neuron replacement is a separate field involving laboratory-derived dopaminergic progenitor cells placed into specific brain regions. UC-MSC or MSC-based supportive therapy is usually discussed differently. The proposed role is more related to secretome signaling, immune modulation, trophic support, and microenvironmental regulation.
For this reason, a high-quality article should not claim that MSC therapy directly replaces lost dopaminergic neurons. A better explanation is that regenerative signaling may support surviving dopaminergic circuits by reducing inflammatory stress, supporting mitochondrial resilience, and improving the biological environment around remaining neurons.
This distinction helps the article appear more medically credible and less similar to generic “stem cells regenerate dopamine cells” content on Google.
Mechanism 6: Tyrosine Hydroxylase as a Research Marker
Tyrosine hydroxylase is the rate-limiting enzyme involved in dopamine synthesis. In Parkinson’s disease research, it is often used as a marker related to dopaminergic neuron integrity or activity in experimental models.
This is a useful mechanism to mention, but it must be handled carefully. Stem cell therapy bangkok thailand for Parkinson’s disease should not be claimed to directly restore tyrosine hydroxylase activity in human patients. A more accurate statement is that regenerative strategies may be evaluated in preclinical models using markers such as tyrosine hydroxylase expression, dopaminergic neuron survival, and striatal signaling.
This section adds scientific depth without overclaiming. It also gives the article a more original angle because most SEO articles avoid specific molecular markers.
Mechanism 7: Autophagy, Mitophagy, and Cellular Waste Management
Autophagy is the process by which cells degrade and recycle damaged components. Mitophagy is the selective removal of damaged mitochondria. Both processes are important for neuronal survival because neurons are long-lived cells that must manage accumulated stress over time.
In Parkinson’s disease, impaired autophagy and mitophagy may contribute to abnormal protein accumulation, mitochondrial stress, and neuronal vulnerability. Reviews in 2025 continue to highlight autophagy dysfunction as an important part of Parkinson’s disease pathogenesis.
MSC-based secretome signaling may be discussed in relation to cellular resilience, inflammation reduction, oxidative stress modulation, and extracellular vesicle cargo that may influence stress-response pathways. However, it should not be claimed that stem cell therapy directly normalizes autophagy in patients.
A balanced sentence would be: Secretome-based regenerative signaling may be relevant to Parkinson’s disease research because it may interact with inflammatory and oxidative conditions that influence autophagy and mitophagy, but clinical confirmation remains necessary.
Mechanism 8: Neurovascular Unit and Blood-Brain Barrier Stress
Neurons do not function alone. They depend on glial cells, endothelial cells, pericytes, immune mediators, vascular tone, and blood-brain barrier regulation. This network is often described as the neurovascular unit.
In chronic neurodegeneration, inflammation and oxidative stress may affect endothelial function and blood-brain barrier stability. This matters because the brain’s microenvironment depends on controlled communication between blood, immune signals, and neural tissue.
MSC-derived secretome signaling may be studied for its possible effects on endothelial repair, vascular communication, inflammation regulation, and tissue homeostasis. For stem cell therapy Bangkok Thailand content, this mechanism helps make the article more advanced because it explains why neurological care may involve brain-body communication rather than focusing only on dopamine neurons.
Again, this should remain a proposed biological pathway, not a clinical guarantee.
Mechanism 9: Peripheral Immune-Neural Crosstalk
Parkinson’s disease may involve more than the central nervous system. Many patients experience non-motor symptoms such as constipation, fatigue, sleep disturbance, mood changes, pain, and autonomic dysfunction. These symptoms support the idea that Parkinson’s disease may involve broader body-brain communication.
Peripheral immune activity, gut-brain signaling, systemic inflammation, and autonomic changes may influence the neurodegenerative environment. This is one reason modern Parkinson’s disease research increasingly discusses systemic mechanisms rather than only the substantia nigra.
MSC-related signaling may interact with immune-cell populations outside the brain, including T cells, macrophages, dendritic cells, and cytokine networks. This does not prove clinical disease modification, but it provides a more sophisticated rationale for studying systemic regenerative approaches.
For Google reindexing, this kind of mechanism-based section helps separate the content from short, generic Parkinson’s stem cell articles.
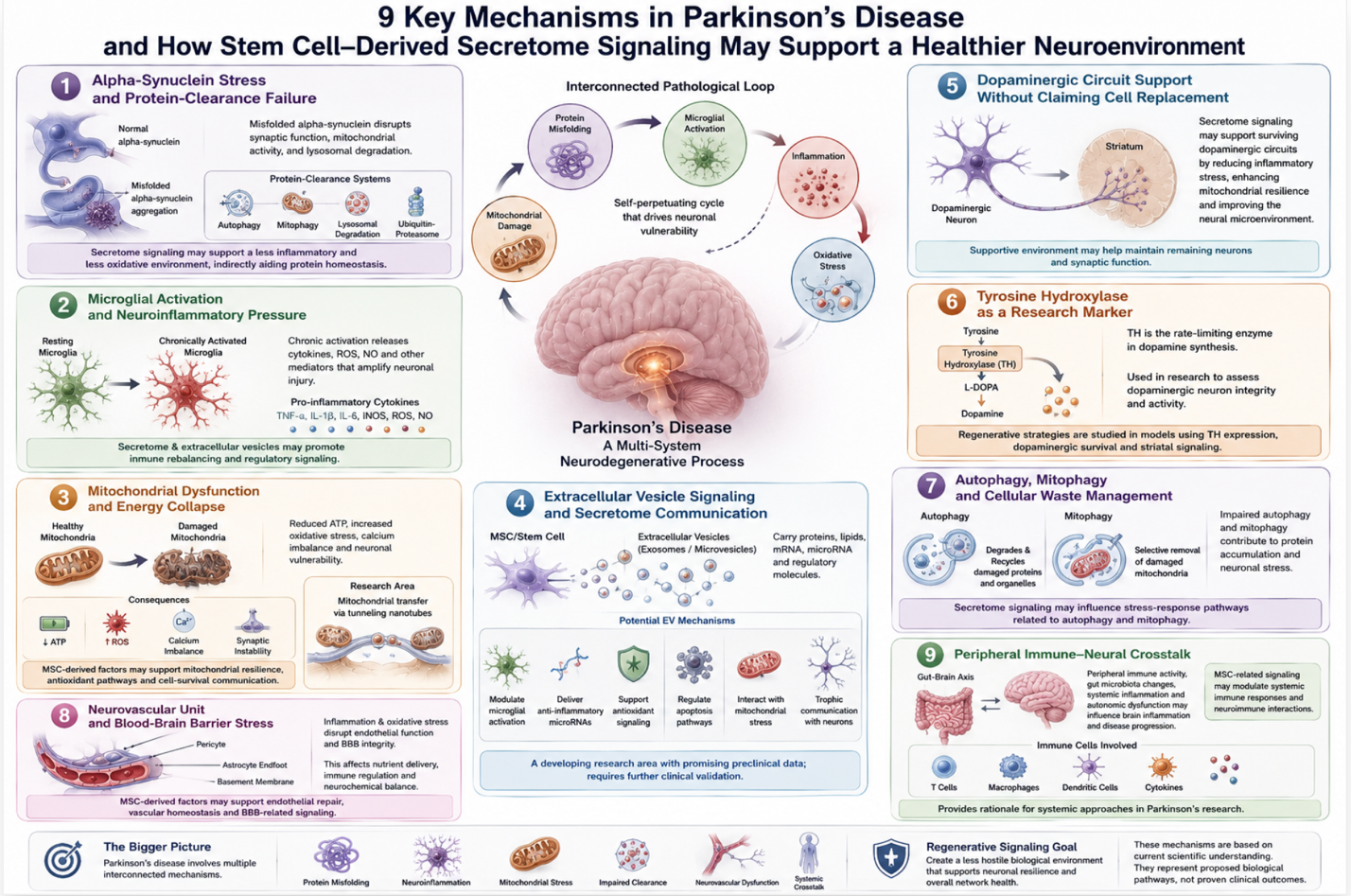
Figure 1: Nine Proposed Neuroprotective Mechanisms of Stem Cell-Derived Secretome Signaling in Parkinson’s Disease
Clinical Positioning for Stem Cell Therapy Bangkok Thailand
Stem cell therapy Bangkok Thailand for Parkinson’s disease should be positioned as physician-guided supportive regenerative care. The strongest clinical angle is not “new cure” or “brain repair breakthrough.” The stronger angle is biological pathway support.
Patients should understand that Parkinson’s disease management still depends on standard neurological care, including medication optimization, physiotherapy, speech therapy, balance training, swallowing assessment, occupational therapy, sleep support, and fall-prevention planning. Regenerative care, when discussed, should sit alongside these foundations rather than replace them.
A serious article should also make clear that outcomes vary. Some patients may report changes in energy, stiffness, movement tolerance, sleep, or rehabilitation participation. Others may experience limited response, especially in advanced disease. Variables such as disease stage, medication response, age, swallowing function, cognition, cardiovascular health, rehabilitation, and treatment protocol may influence outcomes.
Conclusion
Parkinson’s disease is not only a dopamine-deficiency disorder. It is a multi-system neurodegenerative process shaped by alpha-synuclein stress, mitochondrial dysfunction, oxidative injury, impaired autophagy, microglial activation, neurovascular stress, synaptic instability, and immune-neural crosstalk.
A stronger article on stem cell therapy for Parkinson’s disease should focus on these mechanisms rather than repeating generic explanations of what UC-MSCs are or how stem cell therapy is delivered. The more advanced discussion is about secretome signaling, extracellular vesicle communication, inflammatory tone, mitochondrial resilience, protein-clearance stress, tyrosine hydroxylase research markers, and the biological environment surrounding vulnerable dopaminergic circuits.
These mechanisms provide a scientific rationale for why MSC-based regenerative medicine is being studied in Parkinson’s disease. However, they should be presented as supportive and investigational pathways, not as proof of cure or disease reversal.
For patients considering stem cell therapy bangkok thailand, the safest and most credible approach is physician-led evaluation, neurological review, careful cell-quality documentation, realistic expectation setting, and continued standard Parkinson’s care.
Responsible regenerative neurology is not about promising to rebuild the brain. It is about understanding the molecular environment of neurodegeneration and exploring how biological signaling may support selected patients within a complete neurological care plan.
FAQ
Why should Parkinson’s disease content focus on mechanisms?
Mechanism-based content is more useful because Parkinson’s disease involves several interacting pathways, including alpha-synuclein stress, mitochondrial dysfunction, neuroinflammation, oxidative injury, impaired autophagy, and synaptic instability. This gives patients a deeper explanation than simple claims about dopamine replacement.
Can stem cell therapy for Parkinson’s disease replace dopamine neurons?
MSC-based supportive therapy should not be described as direct dopamine neuron replacement. Dopamine neuron transplantation is a separate research field. MSC-based approaches are more often discussed through secretome signaling, immune modulation, and microenvironmental support.
What is the role of extracellular vesicles in Parkinson’s disease research?
Extracellular vesicles may carry regulatory molecules such as proteins, lipids, mRNA, and microRNA. In Parkinson’s disease models, MSC-derived extracellular vesicles are being studied for effects on inflammation, oxidative stress, mitochondrial injury, and neuronal survival pathways.
Why is mitochondrial dysfunction important in Parkinson’s disease?
Dopaminergic neurons require high energy to maintain long axonal projections, neurotransmitter cycling, calcium handling, and synaptic signaling. Mitochondrial dysfunction may reduce ATP production and increase oxidative stress, making neurons more vulnerable.
Is stem cell therapy Bangkok Thailand a cure for Parkinson’s disease?
No. Stem cell therapy Bangkok Thailand should not be presented as a cure for Parkinson’s disease. It may be discussed as supportive and investigational regenerative care for selected patients, while standard neurological treatment remains essential.
What makes this article different from generic Parkinson’s stem cell content?
This article focuses on disease-specific mechanisms such as alpha-synuclein stress, autophagy, mitochondrial dysfunction, microglial activation, extracellular vesicle signaling, tyrosine hydroxylase markers, neurovascular stress, and immune-neural crosstalk rather than repeating basic explanations of stem cells.