

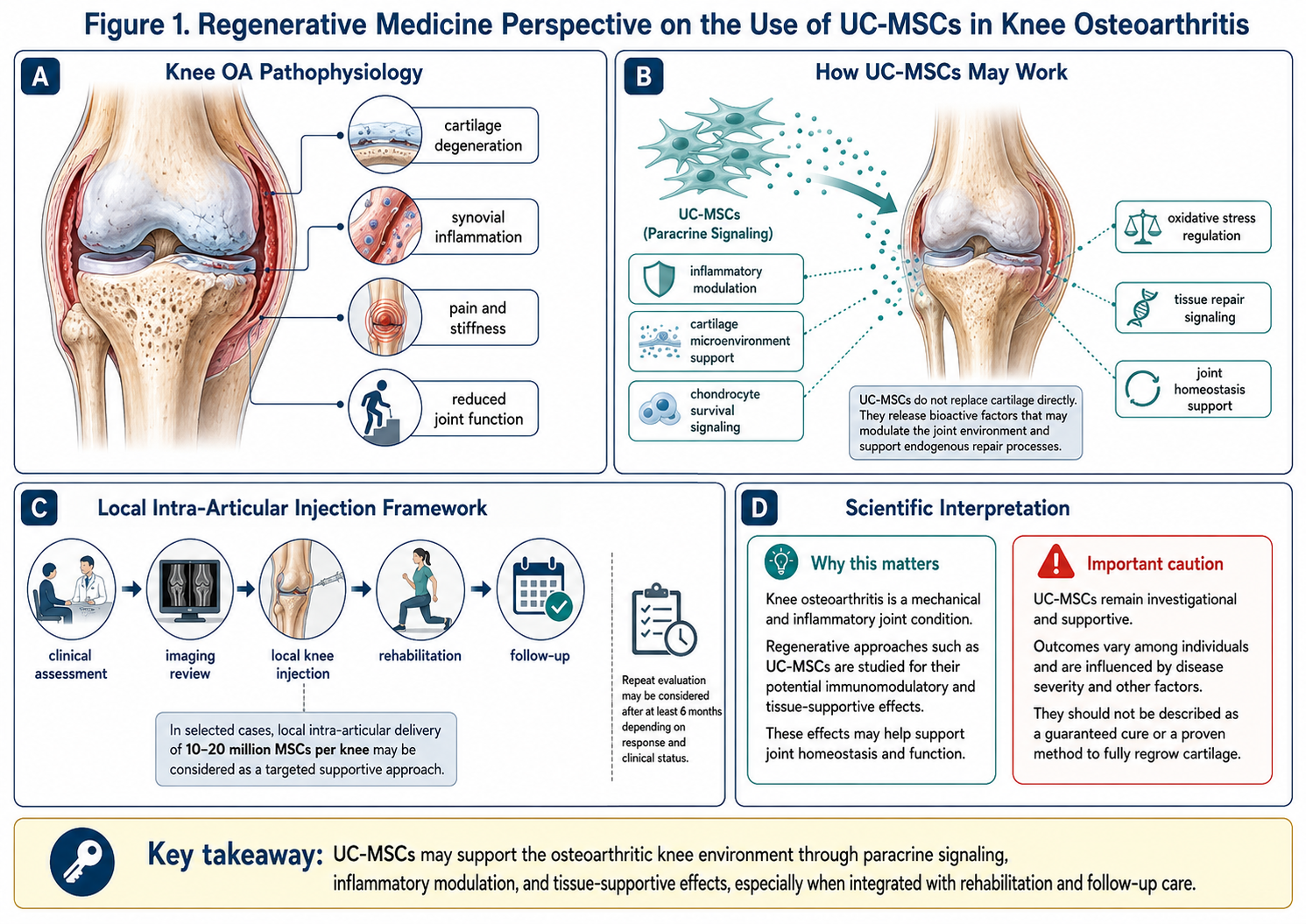
Figure A: Conceptual framework of UC-MSC support in knee osteoarthritis. The proposed mechanisms include paracrine signaling, inflammatory modulation, chondrocyte survival support, cartilage microenvironment regulation, and tissue-repair communication. Clinical response may vary and should be evaluated through imaging review, functional assessment, rehabilitation progress, and follow-up monitoring.
A Closer Look at the Underlying Mechanisms of Knee OA Pain
Knee osteoarthritis (knee OA) is a common type of chronic degenerative joint disease, which includes the loss of cartilage, inflammation in the synovium, subchondral bone remodeling, mechanical overload and progressive aberration of joint function. While many patients think of knee OA as just “knee pain,” there’s a biological process underneath that is far more intricate. This could include inflammatory cytokines, oxidative stress, cartilage matrix breakdown, changes to joint lubrication or progressive immobility.
This is part of the reason why UC-MSC Thailand is a rising search phrase for patients considering regenerative medicine for knee OA treatment. UC-MSCs, or umbilical cord-born mesenchymal stem/stromal cells, have become of interest because they may secrete uncommonly occurring immunomodulatory and tissue-supportive signaling molecules. But this should be budged with pin-point scientific terms. In conclusion, UC-MSCs should not be presented as a panacea for knee osteoarthritis nor described as an established approach to regenerate cartilage advanced methods for full cartilage regrowth.
Discussing UC-MSC Thailand for Knee OA
In Thailand, we developed a reputable image on medical travel, hospital-based care, wellness medicine, international patient coordination and laboratory-supported regenerative programs. UC-MSC Thailand might be attractive to international patients because treatment expense in Thailand is available compared to many Western clinical locations, however it still provides capabilities for physician-guided therapy and organized adhere to-up.
Still, cost should not be the primary motivation for selecting a regenerative plan. In knee OA, quality is king over marketing. An ideal UC-MSC Thailand programme needs to assess clinical presentation including diagnosis, x-ray or MRI findings, OA grade at the concerned joint, pain severity so patients with both background walking ability and background inflammation level need to be stratified; history of previous injections was checked; medication use recorded; body weight and skeletal muscle strength performance were assessed together with rehabilitation exercise programmes.
Investigating the Mechanism Underlying the Role of UC-MSCs in Knee OA
UC-MSCs likely secrete growth factors, cytokines, extracellular vesicles and other bioactive molecules that play a signaling role to nearby joint tissues.
The mechanisms related to MSCs from UC are also being studied because they may influence knee OA by:
inflammatory modulation
synovial inflammation reduction
cartilage matrix support
chondrocyte survival signaling
oxidative stress regulation
tissue repair communication
joint microenvironment balance
pain and functional improvement
Knee OA is not just a mechanical disease, therefore these mechanisms are of scientific interest. A good deal of the pain, swelling, stiffness and tissue break down is resulting from inflammation inside the joint. Intra-articular MSC injection in knee OA has been shown to offer possible clinical benefit, but dose, cell source and preparation, patient selection and study design continue to represent key variables.
At a local knee injection, why 10–20 million MSCs is commonly discussed
In knee OA, due to the direct placement of cells or their signaling activity into the regenerative microenvironment of an affected joint, local intra-articular injection is frequently considered more anatomically precise compared with systemic delivery. In certain examples, a local dose such as ~10–20 million MSCs per knee can be considered and discussed among patients as the lower or higher range of clinically applicable dosing for inflammatory modulation and joint microenvironment support.
A meta-analysis focused on the dose reported that intra-articular MSC therapy was associated with improved clinical outcomes at 12 months for knee OA, in which lower doses of 25 million cells may be effective and possibly more efficient. This again suggests that very high cell numbers might not be always required for any patient, the optimal dose remains to be elucidated.
Logically, from a medical communications perspective, it is better to say that 10–20 million MSCs may support inflammatory balance and cartilage-associated signaling instead of saying it will grow new cartilage. Imaging or cartilage-related improvements have been reported in some studies, but the reproduction of actual cartilage regeneration in human knee OA is variable and should not be expected as a guarantee.
Timing and Repeat Treatment Considerations
Knee OA is a chronic condition; biological response does not happen overnight. Over the course of several months after the local UC-MSC injection, physicians may evaluate pain scores, walking tolerance, swelling, stiffness, range of motion and function. Repeat evaluation can be performed only after at least 6 mos since the initial scan, with a determination of a period based on clinical response, OA burden and imaging results, as well as safety profile.
Not all patients are eligible for repeat injection obviously. Ultimately, some patients respond adequately to one treatment plus rehabilitation, weight management and activity modification. Those with advanced OA will need more supportive care and may ultimately require surgical evaluation.
Conclusion
UC-MSC and knee OA Treatment Key Channels in Regenerative Medicine This interest is justified, as knee osteoarthritis can cause pain, inflammation, cartilage destruction, and stiffness with even over reduction in quality of life. Local intra-articular injection of 10–20 million MSCs may be proposed as a symptomatic local adjuvant treatment strategy reserved for selected patients, particularly when the therapy is aimed at inflammatory modulation and support of the cartilage microenvironment in functional improvement.
But UC-MSCs should not be touted as a definitive way to cure anything or an undeniable means to regenerate cartilage in its entirety. With respect to an appropriate paper-style explanation, one could suggest that UC-MSCs provide paracrine support for the joint environment through delivery of anti-inflammatory cytokines and tissue repair communication, and effects on clinical outcome are dependent upon OA grade, patient selection, injection technique/rehabiltitation and long-term monitoring.