

- Why does this topic keep coming up
When people hear the phrase Natural Cellular Regeneration, they often imagine the body simply “growing new cells” and repairing itself in a clean, almost automatic way. It is an attractive idea, especially in regenerative medicine. But in real biology, the process is more layered than that. Tissue recovery depends on signaling, inflammation control, blood supply, immune balance, extracellular matrix remodeling, and the behavior of the cells introduced into that environment. That is exactly why UC-MSCs have become such a major topic. They sit at the intersection of repair biology, immune modulation, and allogeneic cell therapy in a way that sounds simple on the surface, but is actually technically demanding underneath.
What makes the conversation even more interesting is the role of the stem cell donor. In public-facing discussions, donor issues are often treated like background logistics, as though once a lab says “umbilical cord-derived,” the science has already been settled. It has not. In practice, donor selection, donor screening, donor consent, infectious disease testing, traceability, and product characterization all shape whether a UC-MSC product is merely marketable or genuinely credible. That is why any serious explanation of Natural Cellular Regeneration and UC-MSCs has to spend time on the donor side of the story.
What “Natural Cellular Regeneration” really means
- It is a biological framework, not a magic phrase.
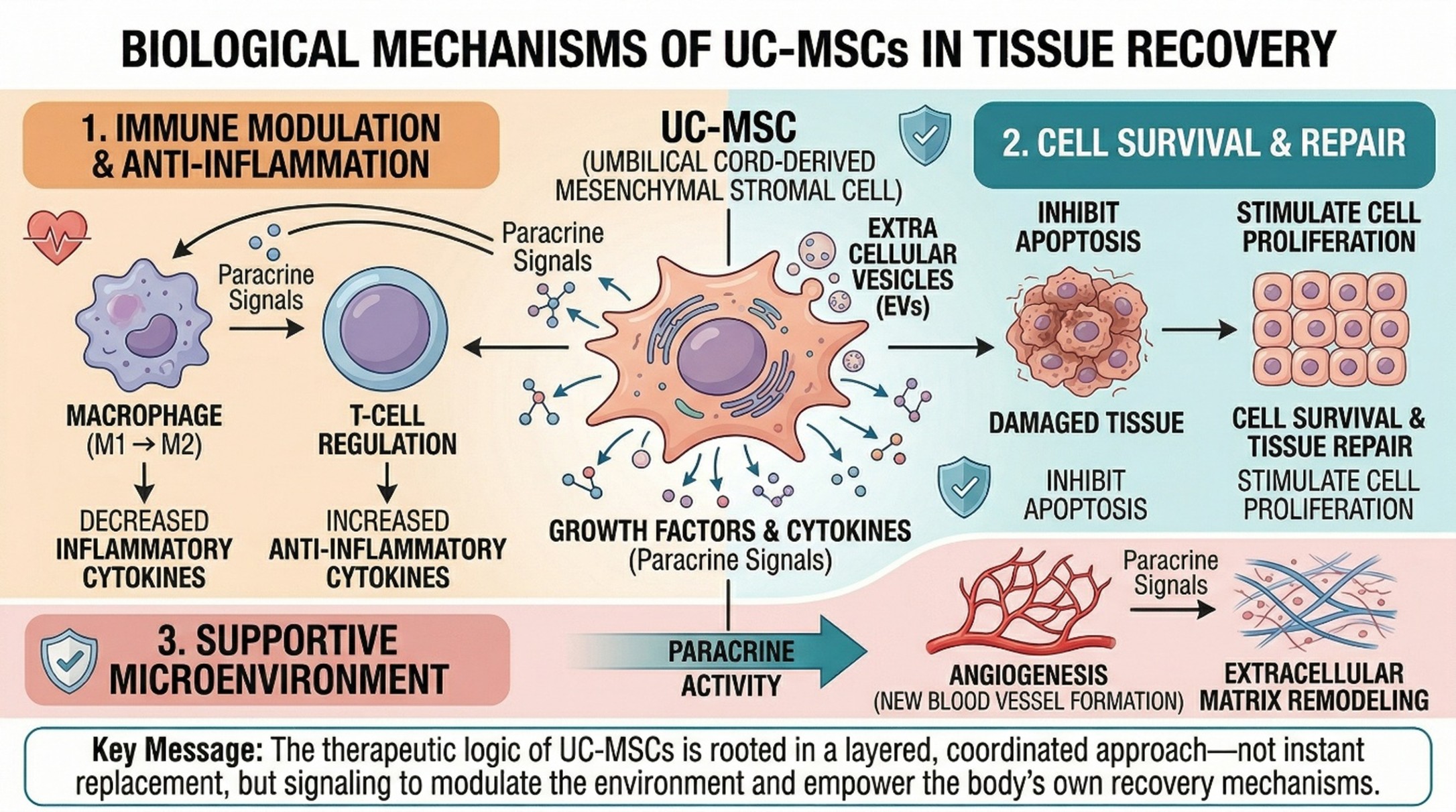
The strongest way to use the term Natural Cellular Regeneration is to treat it as a biological framework rather than a miracle slogan. In MSC science, the therapeutic logic is not only that cells can differentiate. It is also that they can shape the local environment by releasing growth factors, cytokines, and extracellular vesicles while interacting with immune cells and promoting tissue repair, angiogenesis, and cell survival. That is a more accurate picture of regeneration: not instant replacement, but coordinated support for recovery.
This matters because people often assume that regenerative medicine works by “putting in new cells” and letting the body do the rest. In reality, modern MSC literature describes a broader mechanism. MSCs are studied for their immunomodulatory effects, their anti-inflammatory signaling, and their ability to influence tissue microenvironments through paracrine activity as much as through direct engraftment. That is one reason UC-MSCs have drawn so much attention in the first place.
What UC-MSCs are, exactly
- UC-MSCs usually come from umbilical cord tissue, often Wharton’s jelly.
UC-MSCs stand for umbilical cord-derived mesenchymal stromal or stem cells. In most discussions, this refers to MSCs isolated from umbilical cord tissue, especially Wharton’s jelly, the gelatinous connective tissue surrounding the umbilical vessels. The International Society for Cell and Gene Therapy’s classic minimal criteria for MSCs still anchor the field: these cells are expected to be plastic-adherent in culture, to express markers such as CD73, CD90, and CD105, to lack hematopoietic markers, and to demonstrate osteogenic, chondrogenic, and adipogenic differentiation under in vitro conditions.
This website has become so significant for practical reasons. There are many adult-tissue MSC sources. Umbilical cord-derived cells have their unique advantages. They are, generally speaking, because the tissue is commonly discarded after birth and MOU are retrieved at dentist heparin-fibrotic abdominal and notably superficial operations also do not destroy living cells comma refraining from premolar extraction after lower-level formativeness leads to earlier onset with relatively less potential damage near cultural brain level. The reviews of 2025 give an unchanging assessment of perinatal MSCs that their proliferative capacity is stronger than adult MSCs. Later reviews comparing all kinds of MSCs concurred in noting that UC-MSC has particularly strong proliferation with lower immunogenicity.
- Why UC-MSCs are so often linked to regenerative medicine
The phrase Natural Cellular Regeneration links back with the source text. Moving on to the third point of argument about umbilical cord tissue, it is a biologically potent substance. According to the reviews, UC-MSCs are cells that can migrate toward injured or inflamed tissue and participate in immune regulation and support tissue repair. Research has been carried out in all the above inflammatory, autoimmune, metabolic, neurological, pulmonary, and orthopedic disorders, although the level of evidence still varies widely between disciplines. Therefore, swelling over UC-MSCs is not entirely unfounded. Yet it shouldn’t be confused with sweeping one hundred percent endorsement across all categories of illness, either.
Why the stem cell donor matters so much
- A “good source” still depends on a good donor pathway
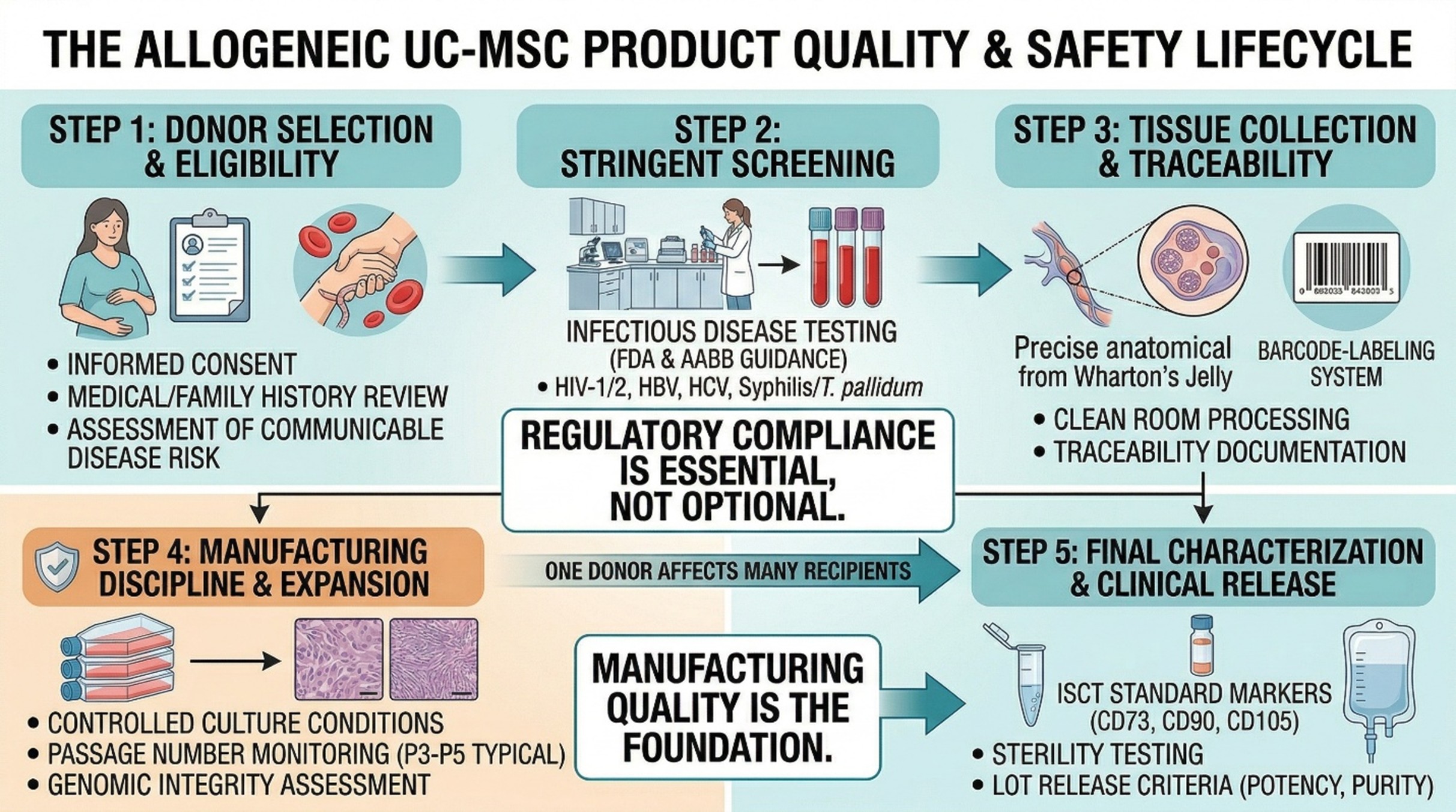
This is the part many people underestimate. Saying that a product uses umbilical cord tissue does not, by itself, tell you enough. The stem cell donor side matters because a donor-derived biologic is only as trustworthy as the system used to collect, document, screen, and release it. FDA guidance for human cells, tissues, and cellular and tissue-based products makes donor eligibility a formal regulatory issue, requiring donor screening and testing. AABB materials likewise emphasize donor screening, infectious disease testing, and the broader donor-eligibility process.
In umbilical cord banking and allogeneic use, this usually means more than a single checkbox. Published banking workflows describe written informed consent from the mother, medical and family history review, assessment of communicable disease risk, maternal blood testing for infections, and continued documentation to preserve traceability. Some systems also include follow-up maternal testing to reduce concern about infections that may have been in the window period at delivery. That may sound administrative, but it is actually central to product safety.
- Infectious disease screening is not an optional detail.
The stem cell donor conversation becomes especially concrete when infectious disease testing enters the picture. FDA donor-eligibility guidance explicitly frames donor screening and testing as required components of HCT/P safety oversight. AABB guidance for cellular-therapy donor eligibility lists infectious disease testing for HIV-1/2, HBV, HCV, and Treponema pallidum among core requirements. In other words, donor screening is not a marketing add-on. It is part of what separates a serious cell-therapy supply chain from a weak one.
- One donor can affect many recipients.
This is another reason donor quality matters more in allogeneic UC-MSC work than many people realize. In published cord-banking discussions, one qualified umbilical cord donor may contribute master cells and derived products for multiple recipients. That makes the consequences of weak screening larger, not smaller. A problem at the donor level can propagate through a much wider treatment network than people assume. For that reason, allogeneic biobanking frameworks emphasize traceability, documentation, and strict safety testing, not just cell expansion.
- Donor quality is only the beginning.
Natural Cellular Regeneration also depends on manufacturing discipline.
Even an excellent stem cell donor does not guarantee an excellent final product. The next layer is manufacturing quality. For years, scientists of MSC have been struggling against the artificial variability introduced by such things as the source of tissues, culture conditions, passage number, measures of efficacy, and the quality of clinical documentation. A review says that when it comes to characterizing UC-MSC, passage can lead to altered purity, growth, and senescence, and genomic integrity and immunomodulation behavior is altered. In contrast, ISCT’s work for clear standards in nomenclature and reporting continues. So if the donor is the base, manufacturing becomes the foundation that is laid on top of it; both are important.
That is the most realistic way to talk about Natural Cellular Regeneration and UC-MSCs. The field is promising because biology is real. Umbilical cord-derived MSCs are genuinely interesting cells with meaningful translational potential. But the credibility of any UC-MSC product depends on a chain of quality that begins with donor consent and donor screening, continues through infectious disease testing and traceability, and extends into characterization, processing, storage, and release criteria. That may sound less romantic than the phrase “natural regeneration,” but it is how regenerative medicine becomes trustworthy.
- Conclusion
The honest conclusion is not that UC-MSCs are overhyped, and it is not that they are a universal answer either. It is that they occupy a serious and fast-developing space in regenerative medicine because of their biology, accessibility, and suitability for allogeneic applications. But the more scalable a donor-derived product becomes, the more important the stem cell donor pathway becomes as well. In other words, Natural Cellular Regeneration starts long before administration. It starts with who donated, how that donation was screened, and whether every step afterward was handled with scientific discipline.
Frequently Asked Questions
1) What is UC-MSCs?
UC-MSCs are mesenchymal stromal/stem cells derived from umbilical cord tissue, most commonly from Wharton’s jelly. They are defined in the literature by accepted MSC criteria involving culture behavior, marker expression, and in vitro differentiation capacity.
2) Why are UC-MSCs often discussed in Natural Cellular Regeneration?
Because MSCs are studied not only for differentiation, but also for immune modulation, anti-inflammatory signaling, and support of tissue repair through secreted bioactive factors. That makes them highly relevant to how people describe regenerative support at the cellular level.
3) Why does the stem cell donor matter so much?
Because donor-derived cell products must begin with a safe and well-documented source. Donor eligibility, informed consent, medical history review, infectious disease testing, and traceability all shape whether an allogeneic UC-MSC product is credible and safe enough to move forward.
4) What kinds of donor screening are usually involved?
Regulatory and accreditation frameworks describe donor screening plus infectious disease testing. AABB donor-eligibility material specifically lists testing for HIV-1/2, HBV, HCV, and Treponema pallidum, while published cord-banking workflows also describe maternal history review and communicable-disease risk assessment.
5) Does a qualified stem cell donor guarantee a high-quality product?
No. Donor quality is essential, but it is only one part of the chain. Product quality also depends on culture conditions, passage number, sterility controls, characterization, storage, and the broader manufacturing system used to produce the final UC-MSC product.