

Globally, women’s health is inextricably linked to women’s reproductive health. Premature ovarian insufficiency (POI) is one of the more serious endocrine disorders, as it disrupts hormonal homeostasis in women before the age of 40. Women with POI suffer devastating effects during the course of their lives including premature infertility, and is associated with depressive symptoms and the effects of accelerated aging. Many of the effects of POI are unfortunately physical and can include vasomotor symptoms and reductions in bone mineral density. The temporary restoration of homeostasis through state-of-the-art regenerative medicine is a viable means of addressing the overwhelming effects of POI. As compared to traditional medicine which treats conservative symptoms, the modern regenerative stem cell clinic seeks to restore the ovarian reserve and address the cellular depletion through the use of UC-MSCs (umbilical cord – mesenchymal stem cells) to those constituents of the ovarian reserve. Through the use of modern regenerative therapies we hope to offer our patients comprehensive homeostatic restoration along the reproductive continuum at our clinic as compared to temporary palliatives.
Mechanisms of Cell Therapy
Cellular therapies at a stem cell clinic depend on many complex, interrelated biological systems that require coordination for successful outcomes when treating Premature ovarian insufficiency. UC-MSCs (umbilical cord – mesenchymal stem cells) show an inherent ability to migrate to sites of ovarian injury due to their novel use of chemokine receptors. Upon arrival to the injured tissue microenvironment, the UC-MSCs take an active role in tissue repair through secretion of a variety of growth factors, cytokines, and vesicular transport systems which are collectively known as the secretome. The primary mechanism of tissue repair is paracrine signaling. The secretome acts to control and modify inflammation in the ovarian stroma. The paracrine factors also stimulate the proliferation of granulosa cells of ovarian follicles.
The restoration of the follicular microenvironment by UC-MSCs halts the apoptosis of key reproductive cells in women with Premature ovarian insufficiency. The consequence of this are the repair and the restoration of the structural integrity of reproductive organs and the proper maturation of endogenous follicles. The remodeling of the environment is the primary characteristic of the regenerative potential observed in the practices of modern medicine at any advanced stem cell clinic.
Limitations of present standard therapies and their drawbacks
For a long time, the only treatment available to physicians for managing deficiencies of the endocrine system was hormone replacement therapy. The administration of external estrogens and progesterone helped to alleviate the bothersome symptoms of menopause such as hot flashes and mood instability. Nonetheless, these therapies offer very little for the long-term restoration of reproductive function. The replacement of hormones does not restore the depleting of follicles in patients with Premature ovarian insufficiency. There is an increased risk of cardiovascular and other endocrine-related complications with a continued use of synthetic hormones. From the standpoint of restorative fertility therapies, the traditional pharmacological therapies are inadequate. These therapeutic gaps are the impetus for the development of new regenerative therapies. Therefore, the symptomatic treatment of these patients in a dedicated stem cell clinic using UC-MSCs is the rational next step.
Justification for use of advanced regenerative UC-MSCs therapy
The shift towards advanced regenerative medicine at a stem cell clinic is due to the unique biological characteristics of UC-MSCs that are derived from the umbilical cord. Compared with other cellular sources, the use of these cells is advantageous due to their higher proliferation and less immunogenicity. These cells are potentially able to stop the progression of Premature ovarian insufficiency by rescuing ovarian follicles that are already compromised. The primary mechanisms of this therapeutic intervention is angiogenesis through a paracrine effect mediated by vascular endothelial growth factor. Vascularization aids in delivering nutrients to starving ovarian tissues affected by Premature ovarian insufficiency. Also, the immunomodulatory feature of UC-MSCs provides defense for the remaining follicles against the autoimmune destructive processes observed in this condition. By modulating the local immune response, the microenvironment favors the growth of follicles. Any high quality stem cell clinic that focuses on regenerative endocrinology will know that the results of these therapies (compared to more temporary, pharmacological, and palliative solutions) are based on these impressive paracrine effects.
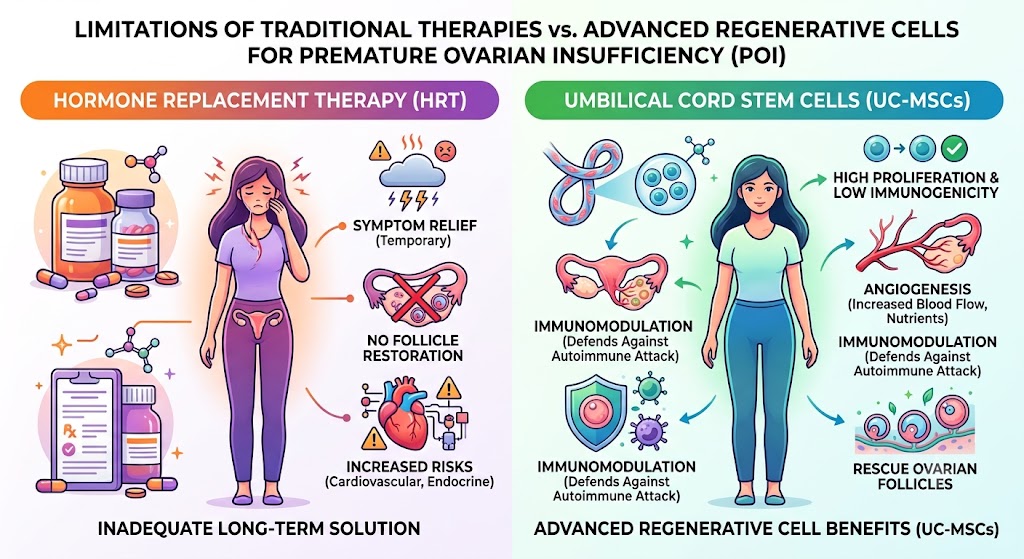
Figure 1: Limitations of present standard therapies compared with advanced regenerative UC-MSCs therapy for ovarian insufficiency
Trends related to the use of UC-MSCs at a stem cell clinic for Premature ovarian insufficiency in the Thailand
The practice of medicine in the Southeast Asian region is beginning to embrace a more regenerative approach. In this setting, for example, the treatment of Premature ovarian insufficiency using advanced cellular therapies has great potential. Thailand is emerging as the lead country for more innovative therapies based on the excellent state of their medical and biotechnological research. Thailand has strong and reliable regulations in the area of cellular therapies, which has attracted patients from around the world to their high-quality private stem cell clinic facilities to receive therapies that are more advanced and less expensive than similar clinics in Western countries. In addition, the warm climate and the country’s great hospitality create an excellent environment for the recovery of international patients. Thai research institutions are conducting numerous clinical trials to evaluate the use of UC-MSCs for reproductive-related disorders. Thailand will most likely be the world leader in regenerative gynecological medicine over the next ten years. It is clear that modern approaches to endocrine disorders such as Premature ovarian insufficiency at a specialized stem cell clinic using UC-MSCs are required. Current approaches to this disorder that only palliate symptoms are clearly insufficient.