

Liver inflammation is usually quite silent until blood tests, ultrasound, FibroScan or symptoms suggest that there might be something going on. Some patients present first with aminotransferase elevation (ALT or AST). Some are told they have fatty liver, an inflammation related to hepatitis, autoimmune liver disease, fibrosis or early cirrhosis.
That’s why there are so many patients look upon stem cells, Stem Cells Therapy and Modulating Liver Inflammation in Thailand. They are not just asking if treatment A can cure the liver. They want to see if the constant inflammatory environment within the liver can be soothed, whether fibrosis progressions can slow up and how remaining liver function may better supported.
The responsible response is cautious: UC-MSC therapy represents a promising area of research; however, it cannot be characterized as a cure for liver disease, an alternative to hepatology care or an unequivocal vehicle to the resolution of cirrhosis.
Why Liver Inflammation Matters
The liver is an ideal organ for reducing the concentration of active compounds in blood circulation because it plays roles in nutrient processing, detoxification including drug metabolism, homeostasis through metabolic regulatory pathways along with factors necessary to support immune surveillance and production of secreted products. For example, the immune system could remain activated due to chronic stimulation by multiple mechanisms like repeated liver injury from fat accumulation (non-alcoholic fatty liver disease), alcohol consumption or viral hepatitis/autoimmune activity and stress of medications/toxins/metabolic diseases.
With time, chronic inflammation may lead to oxidative stress, microangiopathy and hepatocyte damage with activation of hepatic stellate cells. This activation of stellate cells is essential because this action contributes to fibrosis, or the formation of scar-like tissue within the liver.
Once fibrosis is severe, complete structural recovery can be difficult. So, while full “organ regeneration” is a distant goal, targeting the drivers of inflammation to protect existing function and minimize ongoing damage would be much nearer realistic targets.
How UC-MSC stem cell May Be Discussed
Due to their paracrine signaling properties associated with anti-inflammatory and reparative pathways, they are studied in the context of umbilical cord-derived mesenchymal stem cells (UC-MSCs). Such signals could be in the form of cytokines, growth factors or extracellular vesicles as well as other paracrine factors.
The New Improved UC-MSC For Modulating Liver Inflammation Mice: They Don’t Have To Be New. The better description is supportive signaling. In selected patients, UC-MSCs may promote immune balance recently observed with the reported roles of these progenitors in modulating inflammatory cytokine production and activity to support microvascular communication; they also appear to exert effects on fibrotic conditions that favour fibrosis-related pathways.
Hence, stem cell therapy for liver support should be considered as “liver-microenvironment modulation” instead of simply glorified phrases like “growing a new liver.
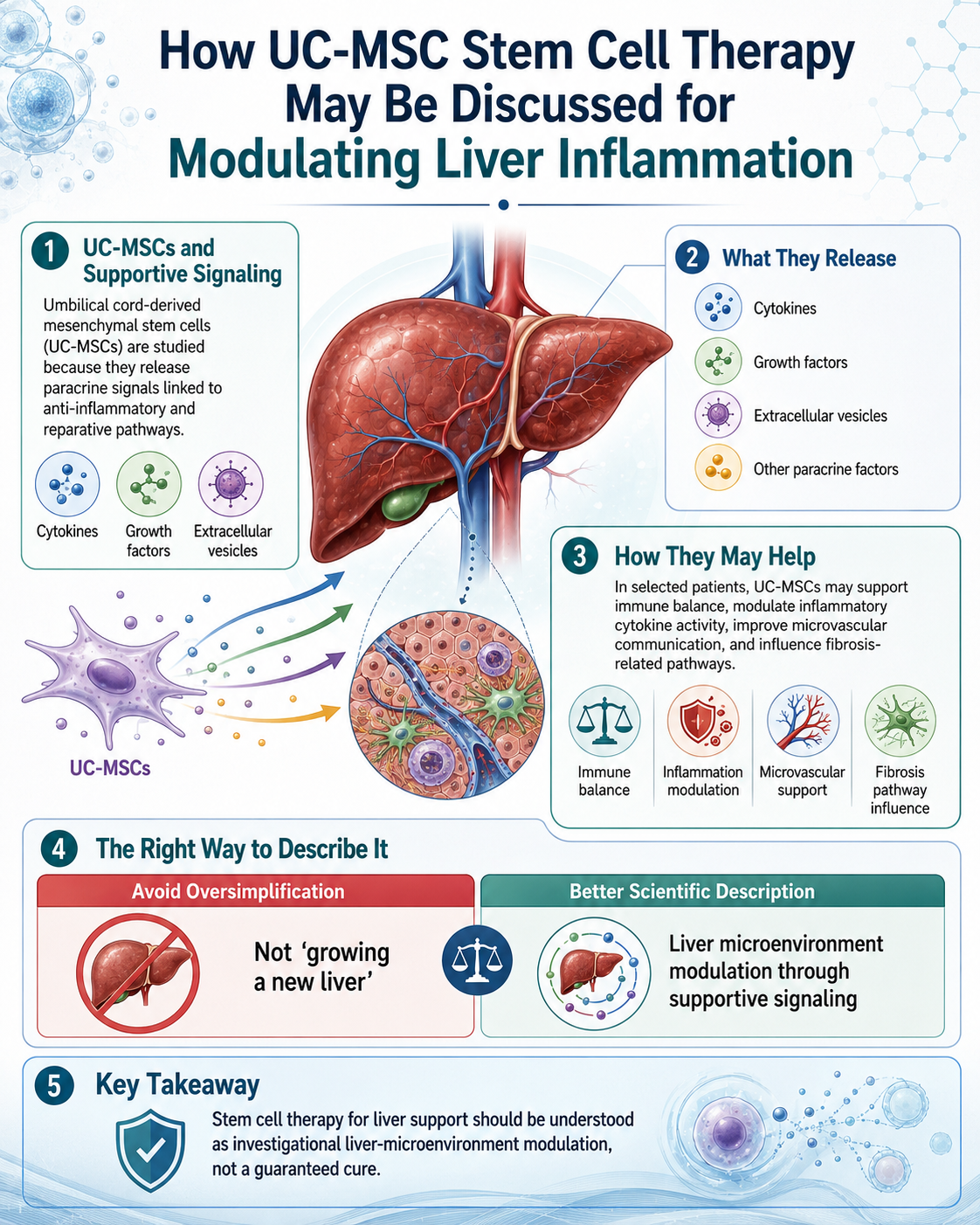
Figure 1: Proposed Supportive Mechanisms of UC-MSC Therapy in Liver Inflammation: Paracrine Signaling, Immune Balance, Microvascular Support, and Fibrosis-Related Pathway Modulation
What Research Suggests So Far
Investigation in MSC-based intervention on chronic and end-stage liver disease is ongoing. Recent reviews suggest that bone marrow and umbilical cord-derived MSCs have great potential because of their immunomodulatory, anti-inflammatory, anti-fibrotic or regenerative signaling effects. There are still significant challenges and limitations in the field with heterogeneous protocols, patient selection, variability in cell source as well as dosage (dose/route/timing safety) and duration of action together with inconsistent outcome comparisons.
Few also assess liver function markers (i.e. ALT, AST, bilirubin, albumin and INR), fibrosis scores, quality of life or complications. Results should be interpreted with caution, nonetheless as liver diseases present a heterogeneous pathology. A patient with fatty liver is not a patient with active viral hepatitis, autoimmune liver disease or decompensated cirrhosis.
Thailand — What Patients Can Expect
What Patients Can Expect from Stem Cell Therapy in Thailand Before stem cell therapy is given, a proper medical review must take place. This can include liver enzymes, bilirubin, albumin, INR, platelet count and hepatitis markers (autoimmune markers), kidney function tests (lipid profile diabetes status ultrasound FibroScan medication history alcohol etc cancer screen & other data regarding hepatologist recommendation).
An ethical clinic should provide information regarding cell source, donor screening for proper risk assessment and infectious disease testing, sterility and viability testing of cells post-production/processing (i.e., endotoxin), route of administration used to expose the patient(s) receiving cellular therapy preparation with details regarding how this is executed [orally/injected] by a physician under direct supervision in case an emergency arises).
Patients should also be informed explicitly that there is variation in outcomes. Examples of reasonable goals include supporting inflammatory balance, enhancing biological readiness, monitoring liver markers and helping the body have a more effective response to standard care.
Standard Liver Care Must Continue
UC-MSC-based stem cell support should be regarded as an adjunct and not replace standard treatment? Depending on disease stage, may require antiviral therapy, alcohol cessation, weight reduction (especially if NASH), diabetes control/lipid management/audience medication/nutrition support/fibrosis monitoring/ liver cancer surveillance / transplant evaluation
In particular, discontinuation of therapy or postponement of hepatology care carries risks in advanced liver disease.
Conclusion
Stem cell therapy for liver inflammation is conceptualized as a novel investigational supportive treatment targeting the balance of the microenvironment at this site. Although these mechanistic pathways driving immune modulation, anti-inflammatory signaling and fibrosis regulation with UC-MSCs can be further studied, they should not yet be touted as a treatment or promise of liver reversal.
For patients considering treatment in Thailand, the only safe approach is diagnosis first (safely confirmed before leaving for Bangkok), documentation of safety second regardless and realistic expectations third (and supported very closely with continued care by an experienced hepatologist ).