

Introduction to the Clinical Challenge
Chronic gastrointestinal inflammation is a global affliction costing millions their quality of life. Crohn’s Disease is amongst the worst. The ongoing abdominal cramping, chronic fatigue, and intestinal obstructions may eventually lead a person to lose weight. Moreover, the psychological toll caused by the relentless nature of an inflammatory illness is significant. Damage to the mucosa of the gastrointestinal tract is a burden and an inconvenience to day-to-day life. It can be unpredictable, further causing distress to the patient. What is needed is a target-focused therapeutic strategy that goes beyond managing symptoms. To achieve sustained remission, a regenerative Stem Cell-based strategy is most encouraging. Interventions involving UC-MSCs will redefine modern gastroenterology. They will cure rather than suppress symptoms by providing a comprehensive immune and structural tissue repair mechanism.
Pathological Mechanisms Underlying the Illness
The host intestinal damage characteristic of Crohn’s Disease is due to a dysregulated immune system response to the intestinal microbiome. The activation and functioning of the T Helper 1 and 17 cells are particularly important. Through the release of an array of inflammatory cytokines, T helper cells facilitate an intense cytokine storm culminating in a continuum of transmural inflammation that affects all layers of the gastrointestinal wall. Chronic inflammation is often compounded by the development of deep mucosal ulcerations and the formation of granulomas. Eventually, re-epithelialization is impeded, and the integrity of the intestinal mucosal barrier is compromised at a microscopic level, allowing bacterial translocation to the lamina propria, necessitating advanced Stem Cell treatments like UC-MSCs.
Such infiltration in Crohn’s Disease perpetuates a pathological cycle of chronic immune hyperstimulation combined with irreversible fibrotic tissue scarring, which Stem Cell therapies using UC-MSCs aim to reverse.
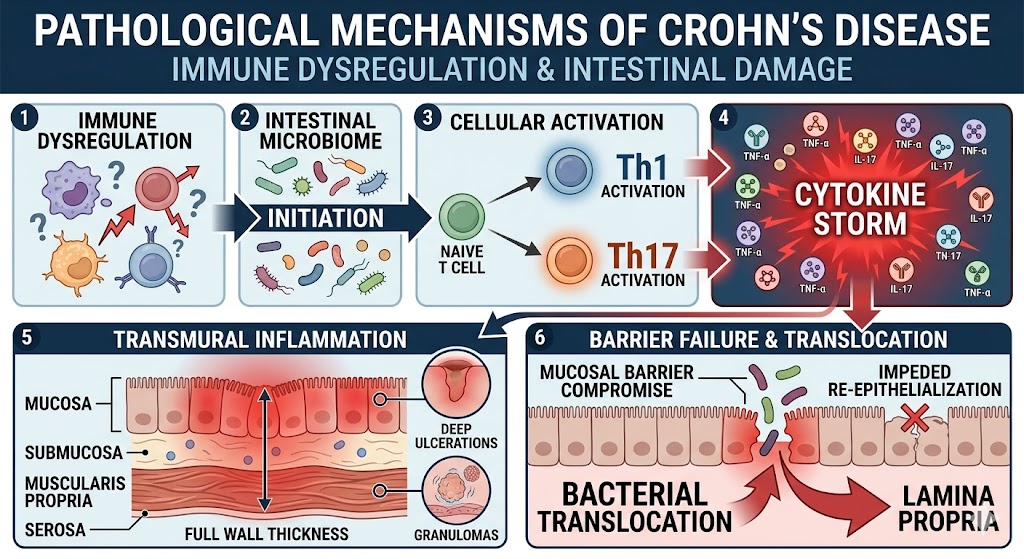
Figure 1: Pathological mechanisms of Crohn’s Disease
Conventional Crohn’s Disease Therapies and Their Limitations
Palliative treatment approaches for Crohn’s Disease involve immunosuppression of a systemic scale. Strong corticosteroids, immunomodulators, or biologic therapies are the therapies of choice. Activated corticosteroids are still the best option for rapidly achieving clinical remission in the case of a flare of acute severity. The eventual reliance on corticosteroids for prolonged periods is bound to cause unwanted effects, such as osteoporosis, metabolic changes, and opportunistic infections. Major improvements in symptomatology for the more responsive individuals are offered by biologic agents that have been developed to target pathways of inflammation. Unfortunately, a large portion of patients develops neutralizing antibodies against these costly biologics. The immunological rejection thus leads to a loss of clinical response. In addition, the highly synthetic medications merely suppress hyperactive immunity for limited periods of time. They do not actually stimulate the healing of the damaged mucosa as an advanced Stem Cell would. An invasive approach through surgical resection of the affected bowel is often the only option available when more conservative medical management has failed, paving the way for UC-MSCs.
Justification for Advanced Cellular Therapeutic Approaches
The failure of conventional immunosuppressants of a systemic scale opens the door for advanced therapeutic approaches targeting the localized stimulation of tissue regeneration. A balanced Stem Cell therapy using UC-MSCs has the potential for delivering true tissue regeneration for Crohn’s Disease. The umbilical cord-derived cells are able to combine their striking Immunomodulatory and high Expansion potential. After their administration via the intravenous route, these cells are able to migrate to sites of active bowel inflammation. Following successful engraftment, these cells are able to secrete a sophisticated paracrine signaling mechanism. The exogenous secretome is composed of Anti-inflammatory cytokines, specialized Growth factors and various Extracellular vesicles. This diverse secretome from UC-MSCs reduces the effectiveness of aggressive effector T-cells in Crohn’s Disease, but increases the expansion of protective T-regs. Additionally, their bioactive Stem Cell secretome stimulates the intestinal resident progenitor niche, leading to the directed epithelial proliferation and restoration of the intestinal epithelium, its tight junctions, and the clearance of pathological scarring, and the deep mucosal healing that no pharmaceutical agent is able to achieve.
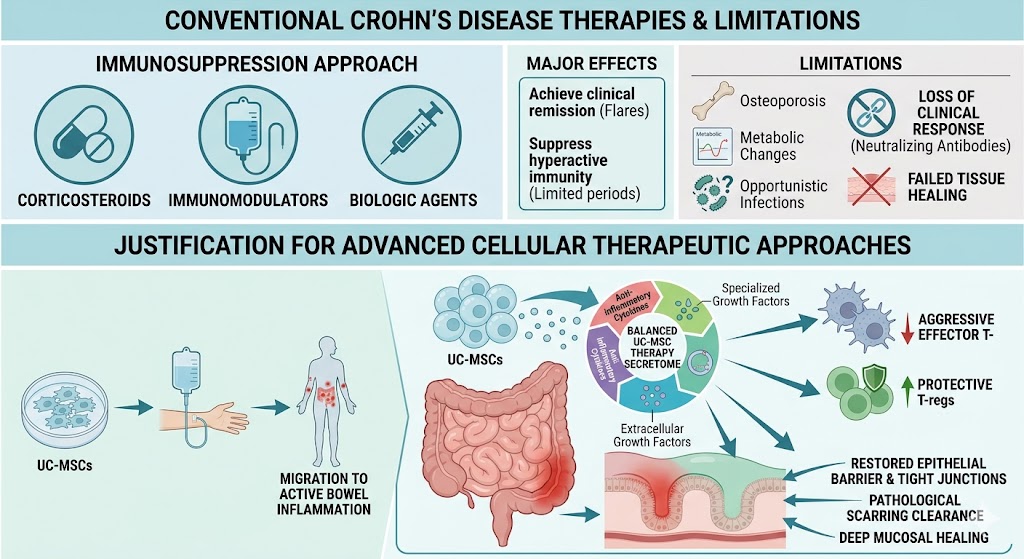
Figure 2: Justification for Advanced Cellular Therapeutic Approaches compared with Conventional Crohn’s Disease therapy
Perspectives for this medical innovation in Thailand
Crohn’s Disease in Thailand has a promising evolving clinical picture due to rapid biotechnology advances in the region. Thailand is trying to be the center for advanced medical innovation in South East Asia. The country now has clinical research centers and regenerative medicine. The Thai public health regulations are increasingly supportive of advanced Stem Cell therapies. This legal trend accelerates the important transition from cell research to regenerative medicine in laboratories and clinical practice. Moreover, the national biobanks are expanding. This important development makes sure there is a consistent, reliable, and high-quality supply of umbilical cord tissue for therapeutic use, specifically for UC-MSCs. The development of a strong local biotechnology industry decreases the dependence on expensive imported biopharmaceuticals. This local biotechnology industry enables Thai patients to receive the most advanced regenerative medicine. The relentless progression of Crohn’s Disease demands innovative therapeutic solutions that go beyond temporary immune suppression. The complex pathogenesis of Crohn’s Disease, especially the severe transmural intestinal inflammation, requires a deep and structural regenerative medicine. The integration of Stem Cell therapies like UC-MSCs represents a substantial innovation in science.
This regenerative Stem Cell therapy targets essentially both restoration of abnormal immune response and restoration of intestinal tissue injury through paracrine mechanisms in Crohn’s Disease. With synthetic drugs showing more operational limits over time, cellular therapy using UC-MSCs becomes more viable as a clinical and biological alternative. With the promise of advanced domestic biotechnological manufacturing in Thailand, innovative regenerative therapies will be available locally to change patients’ prognosis. The pioneering of cellular therapy will, for generations to come, challenge the limits of advanced gastroenterology.