

Stem Cell Therapy for Ulcerative Colitis in Thailand: UC-MSC Stem Cell Therapy Support for Gut Inflammation and Mucosal Healing
Ulcerative colitis, often called UC, is more than occasional stomach discomfort. It is a chronic inflammatory bowel disease that affects the lining of the colon and rectum. During active disease, patients may experience bloody diarrhea, urgency, abdominal cramping, mucus, fatigue, weight loss, anemia, and repeated disruption to daily life.
For some people, standard medication controls the disease well. For others, symptoms return in cycles. A patient may improve for a few months, then flare again. Another may respond to steroids but struggle to stay well without them. Some patients move from 5-ASA therapy to biologics, JAK inhibitors, or other advanced medications, yet still feel that their gut has not fully healed.
This is why many patients search for stem cell therapy for ulcerative colitis in Thailand. They are often not looking for a replacement for their gastroenterologist. They are looking for a supportive approach that may help calm inflammation, support mucosal repair, and improve the biological environment inside the colon.
At Vega Medical Service in Bangkok, UC-MSC stem cell therapy for ulcerative colitis is best understood as supportive and investigational regenerative care. It should not be described as a cure. It should not replace standard IBD treatment, colonoscopy monitoring, prescribed medication, or urgent hospital care during severe flares.
A more responsible way to explain it is this: umbilical cord-derived mesenchymal stem cells, or UC-MSC stem cell therapy, are being studied for their ability to regulate immune activity, reduce inflammatory signaling, support tissue repair pathways, and help create a more balanced environment for gut healing.

Understanding Ulcerative Colitis
Ulcerative colitis is part of a group of conditions called inflammatory bowel disease, or IBD. Unlike Crohn’s disease, which can affect different areas of the digestive tract and deeper layers of the bowel wall, ulcerative colitis usually affects the inner lining of the colon and rectum.
The disease can appear in different patterns. Some patients have inflammation limited to the rectum, known as ulcerative proctitis. Others have left-sided colitis, where inflammation extends further into the colon. Some have extensive colitis or pancolitis, where larger areas of the colon are involved.
The symptoms can vary depending on severity and location. Rectal inflammation may cause urgency, bleeding, and a feeling of incomplete bowel emptying. More extensive inflammation may cause frequent diarrhea, fatigue, fever, anemia, abdominal pain, and weight loss.
One of the most frustrating parts of UC is unpredictability. A patient may look well from the outside but still plan every trip around bathroom access. This daily burden is one reason treatment goals should go beyond simply reducing symptoms. The deeper goal is healing the inflamed lining and helping patients maintain stable remission.
Why Standard UC Treatment May Not Be Enough for Every Patient
Standard ulcerative colitis care may include 5-ASA medications, rectal therapy, corticosteroids, immunomodulators, biologics, small-molecule drugs, nutritional support, and surgery in severe or refractory cases. These treatments are important and can be life-changing.
However, UC can be difficult because inflammation may return even after an initial response. Some patients become steroid-dependent. Some lose response to biologic therapy over time. Some improve symptomatically but still show inflammation on colonoscopy or high fecal calprotectin. Others experience medication side effects or feel that their gut lining remains fragile.
Modern UC care increasingly focuses on objective healing. This means doctors may monitor not only stool frequency and bleeding, but also colonoscopy findings, inflammatory markers, anemia, albumin, and fecal calprotectin.
This is where regenerative medicine becomes an area of interest. Stem cell therapy is not meant to replace proven treatments. Its possible role is to support the biological processes that standard medications may not fully address in every patient: immune regulation, epithelial repair, microvascular support, and tissue recovery.
What Are UC-MSC Stem Cell?
In this article, “UC-MSC stem cell therapy” means umbilical cord-derived mesenchymal stem cells. This should not be confused with “UC,” which also commonly means ulcerative colitis.
UC-MSC stem cell therapy are usually obtained from Wharton’s jelly, the soft tissue inside the umbilical cord, after healthy birth and donor screening. They are not embryonic stem cells. They are also not taken from the patient’s own fat or bone marrow.
UC-MSC stem cell therapy are widely studied because they are young, active in cellular communication, and known for immune-modulating behavior. In inflammatory conditions, their main role is not to become new colon cells after infusion. Their more realistic function is paracrine signaling.
Paracrine signaling means the cells release biological messages such as growth factors, cytokines, extracellular vesicles, and repair-related molecules. These signals may interact with immune cells, inflammatory pathways, blood vessels, and tissue repair systems.
For ulcerative colitis, the aim is not to “replace” the colon lining. The aim is to support a healthier internal environment where inflammation is less aggressive and mucosal healing may become more possible.
How UC-MSC Stem Cell Therapy May Support the Inflamed Colon
Ulcerative colitis involves an overactive immune response in the colon lining. Immune cells release inflammatory signals that damage the mucosa. When this continues, the lining becomes ulcerated, fragile, and less able to absorb fluid properly. This contributes to diarrhea, bleeding, urgency, and pain.
UC-MSC stem cell therapy is being studied because MSC stem cell therapy may influence several pathways at the same time. They may help reduce excessive inflammatory cytokine activity, support regulatory immune cells, influence T-cell and macrophage behavior, reduce oxidative stress, and encourage repair signaling in injured tissue.
This multi-pathway effect is important because UC is not driven by one single molecule. Biologic medications may target specific pathways such as TNF, integrins, IL-12/23, or IL-23. Stem cell signaling is different. It may act more like a biological coordinator, helping shift the immune environment away from chronic injury and toward repair.
However, this should be stated carefully. UC-MSC stem cell therapy is still being studied. It should not be promised to stop all flares, replace biologics, or guarantee mucosal healing.
Mucosal Healing: Why the Colon Lining Matters
Many patients judge ulcerative colitis by symptoms alone. If bleeding improves and bowel movements reduce, they may feel the disease is controlled. Symptoms are important, but they do not always tell the full story.
The colon lining may remain inflamed even when symptoms are quieter. This matters because ongoing inflammation can increase the risk of future flares, anemia, hospitalization, steroid use, and long-term complications.
Mucosal healing means the lining of the colon looks healthier on endoscopy. In modern IBD care, this is an important treatment goal because deeper healing is linked with more stable remission.
UC-MSC stem cell therapy is being studied partly because MSC stem cell therapy may support epithelial repair. The epithelial layer is the barrier between the gut contents and the immune system. When this barrier is damaged, bacteria, food particles, and inflammatory signals may continue to irritate the immune system. Supporting barrier repair may help reduce the cycle of inflammation.
For patients, this means the goal is not only fewer bathroom trips. A stronger goal is a calmer colon lining that is more stable over time.
Who May Consider Stem Cell Therapy for Ulcerative Colitis?
Not every patient with ulcerative colitis is a suitable candidate for UC-MSC stem cell therapy. A more suitable patient may be someone with a confirmed diagnosis, available medical records, stable enough health for treatment, and realistic expectations.
Patients who often ask about regenerative support include those with recurrent flares, persistent inflammation despite medication, steroid dependence, medication intolerance, fatigue linked with chronic inflammation, or interest in supportive care alongside their gastroenterology plan.
More caution is needed for patients with acute severe colitis, toxic megacolon risk, severe dehydration, uncontrolled infection, active gastrointestinal bleeding, severe anemia, unstable blood pressure, suspected colon cancer, or urgent need for hospital care. These situations require immediate gastroenterology or emergency management, not elective regenerative therapy.
Before treatment planning, helpful documents include colonoscopy reports, biopsy results, Mayo score or endoscopic severity score if available, fecal calprotectin, CRP, ESR, hemoglobin, albumin, stool infection results, medication history, biologic history, steroid use, surgery history, and recent imaging.
The clearer the disease profile, the safer and more realistic the treatment discussion becomes.
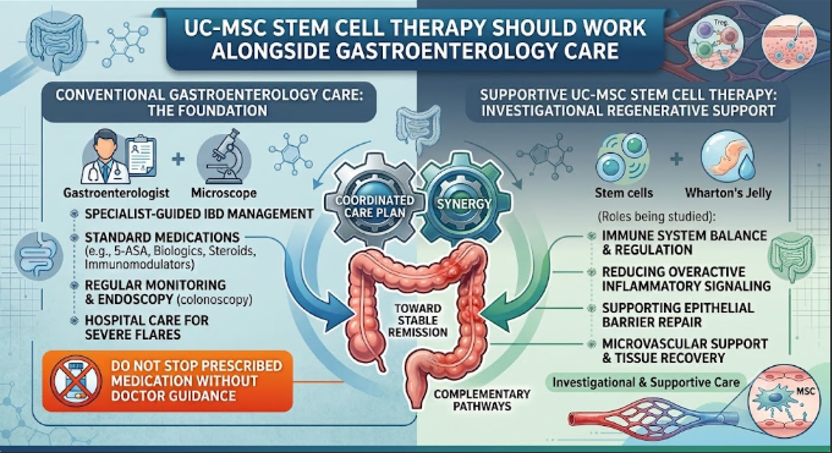
UC-MSC Stem Cell Therapy Should Work Alongside Gastroenterology Care
Patients should not stop their ulcerative colitis medications without guidance from their gastroenterologist. Stopping steroids suddenly can be dangerous. Stopping maintenance therapy can increase the risk of relapse. Delaying urgent treatment during a severe flare can lead to serious complications.
UC-MSC stem cell therapy should be positioned as supportive care, not a replacement for proper IBD management. A patient may still need 5-ASA, rectal therapy, biologics, JAK inhibitors, corticosteroids for induction, nutritional support, iron therapy, or surgery depending on disease severity.
A useful way to explain this is that standard treatment and regenerative support may have different roles. Standard medications aim to control disease activity through established anti-inflammatory pathways. UC-MSC stem cell therapy is being studied for immune balance, tissue repair signaling, and mucosal environment support.
The best plan is coordinated, cautious, and based on objective follow-up.
Why Patients Travel to Thailand for UC-MSC Stem Cell Support
Thailand has become a destination for regenerative medicine because many international patients want coordinated consultation, treatment planning, and supportive care in one trip. For ulcerative colitis patients, travel planning should also consider flare status, diet needs, hydration, medication access, and bathroom comfort.
At Vega Medical Services in Bangkok, UC-MSC stem cell therapy for ulcerative colitis is approached through medical review and realistic expectation-setting. Patients are encouraged to send gastroenterology records before consultation so the medical team can understand disease extent, severity, current treatment, and whether regenerative support has a reasonable role.
The goal is not to replace the patient’s IBD doctor. The goal is to explore whether UC-MSC stem cell therapy may support immune balance and mucosal healing as part of a broader care plan.
Final Thoughts
Ulcerative colitis is a chronic immune-mediated disease that can affect comfort, energy, nutrition, mental health, and daily freedom. Standard gastroenterology care remains the foundation of treatment. Medications, monitoring, colonoscopy, and specialist follow-up are still essential.
UC-MSC stem cell therapy is being studied because of its potential role in immune modulation, inflammation balance, epithelial repair, microvascular support, and mucosal healing. For selected patients, it may be considered as supportive and investigational regenerative care alongside standard treatment.
The right question is not, “Can stem cells cure ulcerative colitis?” A better question is, “What is driving this patient’s ongoing inflammation, how active is the disease, and is there a realistic role for UC-MSC stem cell therapy support within a safe IBD care plan?”
When treatment is guided by medical review, objective monitoring, and honest expectations, regenerative medicine can be discussed responsibly without replacing the care that ulcerative colitis patients still need.