

Stem Cell Therapy for Meniscus Tears in Thailand: A Realistic Guide to UC-MSC Stem Cell Therapy Knee Support
A meniscus tear is one of the most common knee problems, but not every tear behaves the same way. Some tears happen suddenly after a twist, pivot, fall, or sports injury. Others develop gradually from long-term loading, aging, cartilage wear, knee malalignment, or early osteoarthritis.
This is why meniscus treatment should never begin with one fixed protocol. A young athlete with a fresh traumatic tear may need a different plan from an older patient with a degenerative meniscus tear and knee arthritis. Some tears may be treated with rehabilitation. Some may need surgery. Others may be managed with a combination of load control, strengthening, injections, and careful follow-up.
Many patients now search for stem cell therapy for meniscus tears in Thailand because they want to reduce knee pain, improve mobility, and support recovery without immediately choosing surgery when surgery is not clearly required. The responsible discussion is not that stem cells “grow a new meniscus.” A more accurate explanation is that UC-MSC stem cell therapy are being studied for their potential role in inflammation balance, paracrine signaling, tissue microenvironment support, and repair-related communication within the knee.
What the Meniscus Does in the Knee
- The Meniscus Is More Than a Cushion
The meniscus is a C-shaped fibrocartilage structure inside the knee. Each knee has a medial and lateral meniscus. These structures help distribute load, absorb shock, improve joint stability, protect cartilage, and support smooth knee movement.
When the meniscus is torn, the knee may become painful, swollen, stiff, unstable, or sensitive during twisting and squatting. Some patients feel catching, clicking, or locking. Others mainly notice swelling after walking, difficulty with stairs, or reduced confidence when changing direction.
The location and pattern of the tear matter. Tears near the outer vascular zone may have more healing potential than tears in the inner area with limited blood supply. This is one reason treatment planning should be individualized.

Acute Meniscus Tears vs Degenerative Meniscus Tears
- The Cause of the Tear Changes the Treatment Strategy
An acute meniscus tear often occurs after a sudden movement, especially twisting while the foot is planted. This is common in sports and may happen together with ligament injuries.
A degenerative meniscus tear develops more gradually. The meniscus becomes weaker over time, often alongside cartilage stress, early osteoarthritis, reduced muscle support, or long-term loading.
This distinction is important because a traumatic repairable tear may require orthopedic surgical review, especially if the knee locks or remains unstable. A degenerative tear may respond better to structured rehabilitation, activity modification, and joint inflammation control.
A responsible clinic should review symptoms, physical examination, MRI findings, age, activity goals, osteoarthritis stage, and previous treatment before discussing regenerative medicine.
Standard Meniscus Care Still Comes First
- Regenerative Medicine Should Not Replace Orthopedic Evaluation
Standard care for meniscus tears may include rest, activity modification, physical therapy, anti-inflammatory medication when appropriate, bracing, injections, and surgery in selected cases. Orthopedic options may include meniscus repair, partial meniscectomy, or other procedures depending on tear type and knee condition.
Stem cell therapy should not replace proper diagnosis or surgical review when needed. A locked knee, major instability, acute traumatic tear, root tear, large radial tear, severe mechanical symptoms, or combined ligament injury may require orthopedic management.
For patients without urgent surgical indications, regenerative medicine may be discussed as supportive care to help improve the knee environment while rehabilitation continues.
What UC-MSC Stem Cell Therapy Means for Meniscus Tears
- Supportive Biological Signaling, Not Simple Meniscus Replacement
A common misunderstanding is that stem cells are injected into the knee and automatically become new meniscus tissue. In modern MSC stem cell therapy research, the more accurate explanation is supportive biological signaling.
Umbilical cord-derived mesenchymal stem cells, or UC-MSCs, are studied because they can release bioactive signals, including cytokines, growth factors, extracellular vesicles, and other paracrine mediators. These signals may influence how surrounding cells respond to inflammation, tissue stress, and repair demands.
For meniscus tears, UC-MSC stem cell therapy is being explored for its potential to support:
- Inflammation balance inside the knee joint
- Synovial environment regulation
- Fibrocartilage-related repair signaling
- Cartilage protection pathways
- Extracellular matrix communication
- Pain-related inflammatory burden
- Recovery together with rehabilitation and load management
This does not mean UC-MSC stem cell therapy can guarantee meniscus regeneration or prevent surgery in every case. It means they may help support the biological environment in selected patients.
Why Knee Inflammation Matters After a Meniscus Tear
- Pain Is Not Always Only Mechanical
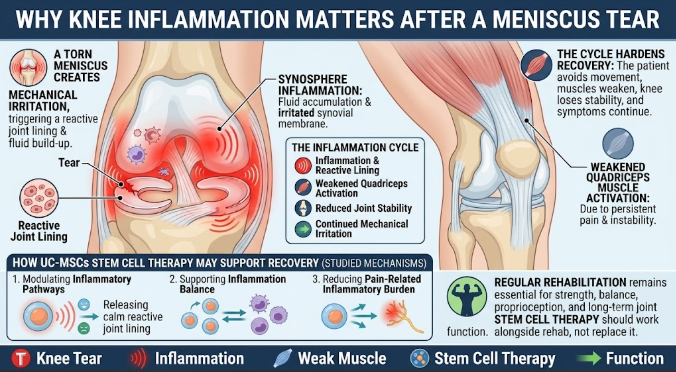
A torn meniscus can create mechanical irritation, but inflammation also matters. After injury, the joint lining may become reactive. Fluid may build up. Cartilage may experience abnormal load. The surrounding muscles may reduce activation because the knee feels painful or unstable.
This cycle can make recovery harder. The patient avoids movement, the quadriceps weakens, the knee becomes less stable, and symptoms continue.
UC-MSC stem cell therapy are being studied because MSC stem cell therapy-related signaling may help modulate inflammatory pathways. In selected cases, reducing inflammatory burden may help the patient participate more effectively in rehabilitation. However, regenerative support should not be described as a mechanical repair for unstable or displaced tears.
Local Knee Injection vs IV UC-MSC Stem Cell Therapy
- Different Routes Have Different Goals
For meniscus-related knee pain, local injection is usually discussed as targeted joint support. It focuses on the knee environment where pain, inflammation, and tissue stress are present.
IV UC-MSC Stem Cell Therapy is generally discussed as systemic support. It may be considered when the patient has multiple areas of inflammation, broader degenerative symptoms, or systemic recovery goals.
Neither route should be presented as automatically superior. The route should depend on diagnosis, symptoms, MRI findings, treatment goals, safety profile, and physician evaluation.
Who May Be a Better Candidate for Discussion?
- Patient Selection Matters More Than Cell Count
Patients often ask how many cells will be used. Cell number is only one part of treatment planning.
Important factors include:
- Tear type and tear location
- Acute or degenerative pattern
- Presence of knee locking or instability
- Cartilage condition
- Osteoarthritis grade
- Meniscus root involvement
- Alignment and loading pattern
- Swelling and synovitis
- Previous injections or surgery
- Rehabilitation history
- Activity goals
- Medical safety profile
A patient with mild degenerative symptoms may have different expectations from a patient with a displaced tear or advanced osteoarthritis. A careful clinic should explain when regenerative support may be reasonable and when orthopedic surgery should be prioritized.
What Patients Should Ask Before Treatment
- Safety and Transparency Are Essential
Before considering stem cell therapy for meniscus tears in Thailand, patients should ask:
- What type of stem cells are used?
- Are they UC-MSC stem cell therapy?
- How are donors screened?
- Are sterility, endotoxin, and viability tests available?
- Will MRI findings be reviewed?
- Is the tear repairable or degenerative?
- Is local injection image-guided when appropriate?
- What are the risks and limitations?
- What rehabilitation plan is recommended?
- How will progress be measured?
Patients should be cautious of clinics that promise a new meniscus, guaranteed surgery avoidance, or rapid return to sport without proper assessment.
Rehabilitation Still Determines Long-Term Function
- The Knee Needs Strength, Control, and Load Management
Even when regenerative medicine is considered, rehabilitation remains essential. Meniscus recovery depends on knee strength, hip control, balance, proprioception, movement quality, and gradual loading.
A proper plan may include:
- Swelling control
- Range of motion work
- Quadriceps and hamstring strengthening
- Hip and gluteal strengthening
- Balance and proprioception training
- Gradual return to stairs, squats, walking, running, or sport
- Load management and activity modification
Stem cell therapy should be discussed as supportive care that works alongside rehabilitation, not as a replacement for it.
How Progress Should Be Measured
- Functional Markers Are More Useful Than Hype
Progress after meniscus treatment should be measured in practical ways, such as:
- Pain during walking or stairs
- Swelling after activity
- Knee range of motion
- Squat depth and control
- Single-leg balance
- Walking distance
- Confidence with turning or pivoting
- Ability to exercise
- Need for pain medication
- Patient-reported knee function
- Follow-up imaging when appropriate
Some patients may notice gradual improvement over weeks to months. Others may have limited response if the tear is mechanically unstable, degeneration is advanced, or rehabilitation is inconsistent.
Conclusion: A Better Way to Discuss Stem Cell Therapy for Meniscus Tears
Stem cell therapy for meniscus tears in Thailand should be discussed with both hope and caution. UC-MSC stem cell therapy are being studied because of their potential role in inflammation balance, paracrine signaling, fibrocartilage repair communication, and joint microenvironment support.
But meniscus tears are not all the same. Some require orthopedic repair. Some respond to rehabilitation. Some are part of a broader osteoarthritis pattern. The best care plan begins with diagnosis, imaging review, patient selection, safety screening, and realistic goals.
For selected patients, UC-MSC stem cell therapy -based support may be considered as part of a broader knee recovery plan. The goal is not to promise a new meniscus. The goal is to support pain reduction, mobility, joint comfort, and long-term function in a medically responsible way.
FAQ: Stem Cell Therapy for Meniscus Tears in Thailand
- Can stem cell therapy heal a torn meniscus completely?
Stem cell therapy should not be presented as a guaranteed way to heal a torn meniscus. UC-MSCs stem cell therapy are being studied for supportive signaling, inflammation balance, and tissue microenvironment support, but outcomes depend on tear type, location, severity, and rehabilitation.
- Who may need surgery instead of stem cell therapy?
Patients with locked knees, unstable tears, root tears, large radial tears, major mechanical symptoms, ligament injuries, or severe joint degeneration may require orthopedic surgical evaluation.
- Is local injection or IV therapy better for meniscus tears?
Local injection is usually more targeted for knee symptoms, while IV therapy is generally discussed as systemic support. The best route depends on the patient’s MRI, symptoms, medical history, and physician evaluation.
- Should physical therapy continue after stem cell therapy?
Yes. Physical therapy is important for strength, balance, range of motion, movement control, and long-term knee function. Stem cell therapy should not replace rehabilitation.
- What should patients prepare before treatment?
Patients should prepare MRI reports, X-rays if available, diagnosis history, pain pattern, swelling history, prior injections or surgery, medication list, and rehabilitation history.