

Stem Cell Therapy for HIV/AIDS in Thailand: UC-MSC Stem Cell Therapy Support for Immune Recovery and Chronic Inflammation
HIV treatment has changed dramatically over the past several decades. With modern antiretroviral therapy, often called ART, many people living with HIV can control viral replication, maintain an undetectable viral load, reduce the risk of transmission, and live longer, healthier lives. For this reason, ART remains the foundation of HIV care.
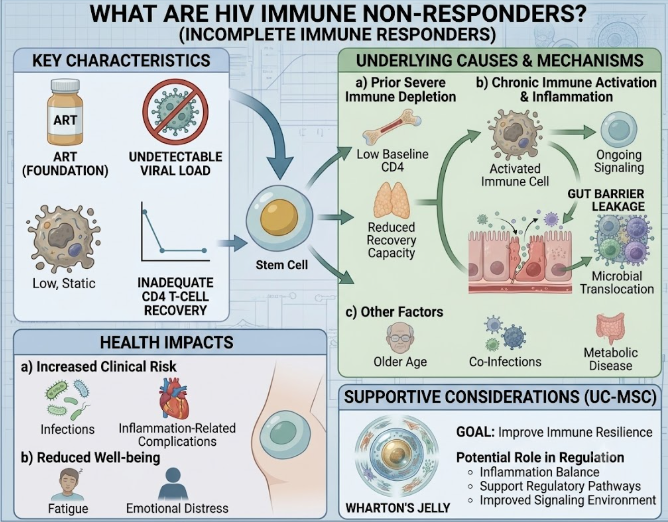
However, not every patient experiences full immune recovery even when the virus is well controlled. Some patients maintain an undetectable viral load for years but continue to have low CD4 T-cell counts, chronic inflammation, fatigue, repeated infections, or slow immune restoration. These patients are sometimes described as immune non-responders or incomplete immune responders.
This is where stem cell therapy for HIV/AIDS has gained scientific interest. Human umbilical cord-derived mesenchymal stem cells, often called hUC-MSC stem cell therapy or UC-MSC stem cell therapy, are being studied for their potential role in immune regulation, inflammation balance, tissue repair signaling, and support of immune recovery.
At Vega Stem Cell Clinic in Bangkok, Thailand, UC-MSC stem cell therapy for HIV/AIDS should be explained carefully. It is not a cure for HIV. It does not remove HIV reservoirs. It does not replace ART. A realistic way to understand it is as supportive and investigational regenerative care that may help selected patients improve immune resilience while continuing standard HIV treatment.
Understanding HIV, AIDS, and Immune Recovery
HIV is a virus that targets the immune system, especially CD4 T-cells. CD4 cells help coordinate immune defense against infections. When HIV is not treated, the virus can gradually reduce CD4 levels and weaken immune protection.
AIDS is the most advanced stage of HIV infection. It may occur when CD4 levels become very low or when certain opportunistic infections or HIV-related illnesses develop. With effective ART, many patients can prevent progression to AIDS or recover immune function after starting treatment.
The main goal of HIV treatment is viral suppression. When viral load becomes undetectable, it means the amount of HIV in the blood is extremely low. This is very important for long-term health and transmission prevention.
However, viral suppression and immune recovery are not always the same thing. A patient may have an undetectable viral load but still have a CD4 count that remains lower than expected. This can leave the patient concerned about long-term immune health.
What Are Immune Non-Responders?
Immune non-responders are people living with HIV who take ART successfully and maintain viral suppression, but their CD4 T-cell counts do not recover adequately. This may happen for several reasons.
Some patients started ART when CD4 levels were already very low. Others may have older age, long-term immune activation, co-infections, metabolic disease, gut immune damage, chronic inflammation, or reduced bone marrow and thymic recovery. The immune system may remain “activated” even after viral load is controlled.
This matters because low CD4 recovery can be linked with higher risk of infections, inflammation-related complications, fatigue, and reduced immune resilience. It can also affect how patients feel emotionally, because they may wonder why their labs are not improving even though they are following treatment correctly.
UC-MSC stem cell therapy is being studied mainly in this type of situation: patients whose HIV is controlled with ART but whose immune recovery remains incomplete.
What Are UC-MSC Stem Cell Therapy?
UC-MSC stem cell therapy are mesenchymal stem cells derived from umbilical cord tissue, commonly from Wharton’s jelly. They are collected after healthy birth with donor screening and consent. They are not embryonic stem cells and are not taken from embryos.
In regenerative medicine, UC-MSC stem cell therapy are mainly studied for their signaling effects. They can release growth factors, cytokines, extracellular vesicles, and other biological messages that may influence immune activity, inflammation, tissue repair, and cellular communication.
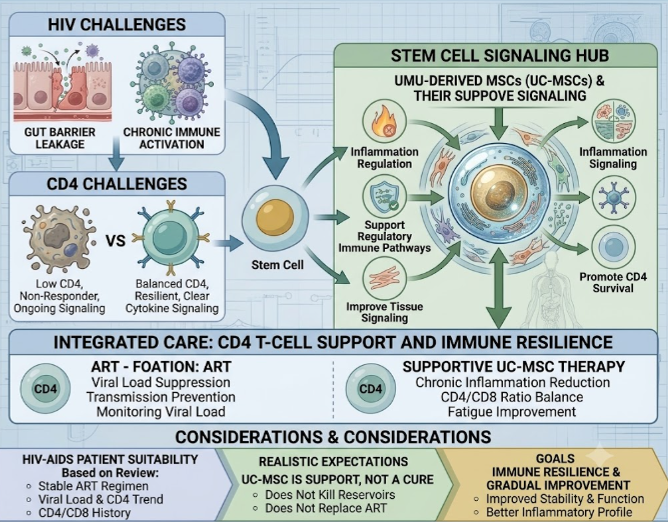
This is called paracrine signaling. In simple terms, UC-MSC stem cell therapy may act more like biological messengers than replacement cells. For HIV immune support, the goal is not for stem cells to attack HIV directly. The goal is to support the immune environment so the body may have better conditions for recovery and regulation.
What Stem Cell Therapy Can and Cannot Do in HIV
This point is very important. UC-MSC stem cell therapy does not kill HIV, remove the virus from hidden reservoirs, or replace antiretroviral medication. Patients should not stop ART because of stem cell therapy.
ART controls viral replication. UC-MSC stem cell therapy, when considered, has a different purpose. It may be explored for immune modulation, inflammation reduction, CD4 recovery support, and general immune resilience in selected patients.
There are rare reports of HIV remission after hematopoietic stem cell transplantation, usually in patients who needed aggressive treatment for blood cancers. That is a very different procedure from UC-MSC stem cell therapy. Hematopoietic stem cell transplant is high-risk, complex, and not used as routine HIV treatment.
UC-MSC stem cell therapy should be positioned as supportive care, not as a cure strategy.
Why Chronic Inflammation Matters in HIV
Even with good viral control, some people living with HIV have ongoing immune activation and chronic low-grade inflammation. This inflammatory burden may affect energy, blood vessels, metabolism, immune function, and general health.
The immune system can remain activated because of previous immune damage, gut barrier changes, co-infections, aging, lifestyle factors, or long-term inflammatory signaling. Over time, this may contribute to fatigue, slower recovery, cardiovascular risk, metabolic issues, or reduced immune stability.
UC-MSC stem cell therapy are being studied because they may help regulate inflammatory signals and support a more balanced immune response. This does not mean inflammation is the only issue in HIV. It also does not mean stem cells can normalize every immune marker. But inflammation balance is one of the main reasons MSC stem cell therapy is being investigated in HIV-related immune non-response.
CD4 T-Cell Support and Immune Resilience
CD4 count is one of the most important immune markers in HIV care. A rising CD4 count after ART usually suggests immune recovery. But in some patients, CD4 numbers stay low or improve very slowly.
Researchers are interested in whether UC-MSC stem cell therapy may support CD4 recovery indirectly by improving the immune environment. Possible mechanisms include reducing chronic immune activation, supporting regulatory immune pathways, improving tissue signaling, and encouraging healthier conditions for immune cell survival.
This does not mean UC-MSC stem cell therapy directly produce CD4 cells. The body’s immune system is complex, involving bone marrow, lymph nodes, gut-associated immune tissue, thymic activity, cytokines, and many types of immune cells. UC-MSC stem cell therapy may support some of these communication pathways, but results can vary.
A realistic treatment goal may be better immune stability, improved inflammatory profile, or gradual improvement in immune markers when combined with consistent ART and medical monitoring.
Who May Consider UC-MSC Stem Cell Therapy for HIV/AIDS Support?
UC-MSC stem cell therapy may be most relevant for patients who are already under HIV medical care and have stable ART treatment. The patient should ideally have an undetectable or well-controlled viral load but incomplete immune recovery, low CD4 counts, chronic inflammation, fatigue, or recurrent immune-related concerns.
A careful review should include:
- Current ART regimen
- Viral load history
- CD4 count trend
- CD4/CD8 ratio if available
- History of opportunistic infections
- Co-infections such as hepatitis B or C
- Kidney and liver function
- Blood counts
- Inflammatory markers if available
- Medication history
- General health and immune-related symptoms
More caution is needed for patients with uncontrolled viral load, active opportunistic infection, untreated tuberculosis, severe liver or kidney disease, active cancer, unstable medical conditions, severe anemia, or recent hospitalization. These cases require specialist medical management first.
UC-MSC Therapy Should Work Alongside ART
ART remains the foundation of HIV treatment. Patients should not interrupt, reduce, or change HIV medication without their infectious disease specialist or HIV doctor.
UC-MSC stem cell therapy should be considered only as an adjunctive support option. This means it may be added to a broader care plan, but it does not replace the medicines that control HIV replication.
This distinction protects patients. If ART is stopped, viral load can rebound, CD4 cells may decline, and resistance risk may increase. A responsible regenerative medicine plan must respect the central role of ART.
Patients should also continue routine HIV monitoring, including viral load, CD4 count, medication safety labs, and screening for co-infections or complications.
Why Patients Travel to Thailand for HIV Immune Support
Thailand has long experience in international healthcare, wellness services, and regenerative medicine. Some patients living with HIV choose Thailand because they want privacy, coordinated consultation, supportive care, and clear treatment planning during a short stay.
At Vega Stem Cell Clinic in Bangkok, UC-MSC stem cell therapy for HIV/AIDS support is approached through medical review, safety screening, and realistic expectations. Patients are encouraged to provide recent HIV labs before consultation, including viral load, CD4 count, ART regimen, blood count, liver function, kidney function, and any history of opportunistic infections.
The goal is not to replace HIV care. The goal is to explore whether regenerative immune support may have a reasonable role alongside stable ART.
Final Thoughts
Stem cell therapy for HIV/AIDS is an evolving area of regenerative medicine. The most relevant discussion is not about curing HIV, but about supporting immune recovery in selected patients who remain immune non-responders despite successful antiretroviral therapy.
UC-MSC stem cell therapy are being studied because of their potential role in immune modulation, inflammation balance, repair signaling, and immune resilience. For some patients, this may be a meaningful supportive concept, especially when CD4 recovery remains incomplete.
However, ART remains essential. UC-MSC therapy should never be presented as a replacement for HIV medication, a guaranteed CD4 booster, or a cure for AIDS. The most responsible question is: “Is the patient virally suppressed, medically stable, and still experiencing incomplete immune recovery that may benefit from supportive regenerative care?”
When treatment is guided by HIV medical records, safety screening, realistic expectations, and continued ART, UC-MSC therapy can be discussed in a safer and more useful way for patients seeking immune recovery support in Thailand.