Chronic Obstructive Pulmonary Disease (COPD) remains one of the leading causes of morbidity and mortality worldwide. Traditionally, clinical management has focused on symptomatic relief through bronchodilators and corticosteroids. However, these treatments fail to reverse the underlying structural damage to the lung parenchyma. As we move through 2026, the application of Umbilical Cord-derived Mesenchymal Stem Cells (UC-MSCs) has emerged as a transformative strategy, moving the goalpost from palliative care to functional alveolar restoration.
The Pathophysiological Challenge: Chronic Inflammation and Tissue Decay
COPD is characterized by persistent airway inflammation and an imbalance between proteases and antiproteases, leading to the destruction of alveolar walls—a condition known as emphysema. This environment is dominated by pro-inflammatory cytokines such as and , alongside high levels of oxidative stress that prevent natural tissue repair.
In a diseased lung, the endogenous repair mechanisms are overwhelmed. The resident progenitor cells become “exhausted,” unable to replace the damaged epithelial lining. This creates a cycle of chronic scarring and declining lung function, measured by a steady decrease in (Forced Expiratory Volume).
The Mechanism: Immunomodulation and Paracrine Signaling
UC-MSCs offer a multi-faceted approach to breaking this cycle. Unlike traditional drugs, these cells act as “biological sensors” that respond to the specific inflammatory markers in the lung.
The primary therapeutic effect is achieved through paracrine signaling, where UC-MSCs secrete a potent cocktail of secretomes and exosomes. Key mechanisms include:
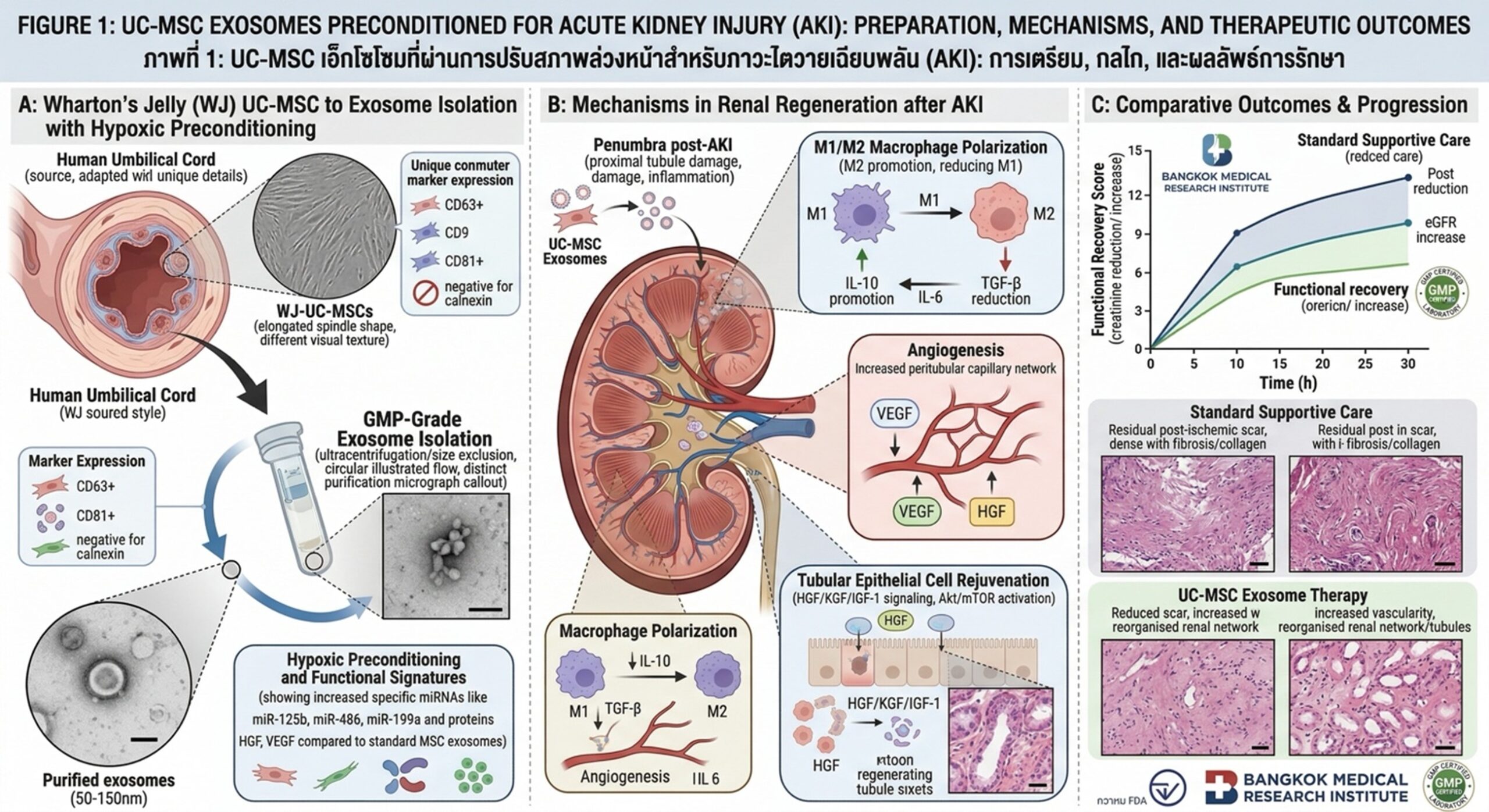
- M1 to M2 Macrophage Polarization: UC-MSCs facilitate the switch of alveolar macrophages from a pro-inflammatory state (M1) to a pro-resolving, reparative state (M2).
- Mitochondrial Transfer: Recent studies in 2026 have highlighted the ability of UC-MSCs to donate healthy mitochondria to damaged alveolar epithelial cells via tunneling nanotubes, effectively “recharging” the cells’ energy production.
- Alveolar Epithelial Repair: By releasing Keratinocyte Growth Factor (KGF) and Hepatocyte Growth Factor (HGF), UC-MSCs stimulate the proliferation of Type II alveolar cells, which are crucial for lung regeneration.
Clinical Delivery: From Intravenous to Inhalation
In the current clinical landscape, the delivery of UC-MSC-derived products has become more refined. While intravenous (IV) injection remains common due to the “pulmonary first-pass effect”—where cells naturally lodge in the lung capillaries—2026 has seen a rise in nebulized exosome therapy.
Note: Nebulized delivery allows the regenerative signals to reach the distal airways directly, bypassing systemic circulation and reducing the risk of off-target effects.
Conclusion: Restoring the Breath of Life
The integration of UC-MSCs into the treatment of COPD represents a monumental shift toward functional restoration. By suppressing chronic inflammation and actively promoting the repair of the alveolar-capillary barrier, this technology offers hope for patients who were previously considered beyond the reach of conventional medicine. As we continue to refine these bio-signaling protocols, the prospect of reversing the structural hallmarks of COPD moves closer to clinical reality.