

Meta Description:Explore how UC-MSCstem cell therapy of knee injections may support selected osteoarthritis patients by targeting synovial inflammation, cartilage stress, subchondral bone changes, and joint microenvironment repair.
Knee pain is widely reported to be a simple explanation of “fuzzy cartilage,” but the explanation isn’t that it. Knee OA is now viewed as a whole-joint disease involving the following structures: cartilage, synovium, subchondral bone, meniscus, ligaments, muscles, inflammatory mediators and biomechanical changes. The knee is not only a hinge. Essentially a living biological system that reacts to pressure, injury, inflammation, weight; movement quality; and the level of cellular stress.
This is significant as patients typically inquire about UC-MSC stem cell knee injections following years of pain pills, physical therapy, steroid injections, hyaluronic acid (HA) injection, platelet-rich-plasma (PRP), or surgical consultation. Some are ineligible for knee replacement. Others have mild to moderate osteoarthritis but would like to preserve the joint. Others have progressed to advance degeneration and want to avoid surgery at any cost.
Regenerative orthopedics has been increasingly investigated for umbilical cord-derived mesenchymal stem cells (UC-MSCs) because of their inherent potential to release biologically active signals resting atop the multitude of potential influences on inflammation, immune regulation, extracellular matrix balance between biosynthesis and turnover, cartilage-cell stress, angiogenic signaling, and joint repair communication. Nevertheless, UC-MSC stem cell therapy must not be touted as either a cure for knee osteoarthritis or proof of how to regrow normal cartilage in every patient.
The type of umbrella that is more medically responsible is this: UC-MSC stem cell therapy of knee injections may benefit the right patient by enhancing the biological milieu of a diseased joint. The goal is not immediate restoration of cartilage, the goal is conservation, symptom relief, modulation of inflammation and improvement of function.
Whole-joint disorder knee osteoarthritis
Osteoarthritis is broader than the cartilage surface. Modern reviews also view OA as the disease of a joint organ; encompassing structural and functional connective-tissue changes in cartilage, subchondral bone, synovium, ligaments, periarticular muscles and inflammatory. Two patients with similar X-ray findings may go through completely different symptoms, which is why. As an example, a patient with moderate cartilage loss may be able to walk comfortably while another may have severe pain from synovitis, bone marrow lesions, meniscus degeneration or poor muscle control.
The knee with OA may have cartilage loss, bone spurs (osteophytes), narrowing of the joint space, hardening of adjacent bone (subchondral sclerosis), synovial inflammation, meniscal extrusion and altered load distribution. Pain mechanisms could involve inflamed synovium, subchondral bone stress, stretched joint capsule or periarticular tendons with nerve sensitization. Because cartilage has a relatively poor blood and nerve supply, pain is most often provoked by the adjacent joint environment rather than isolated cartilage alone.
UC-MSC stem cell therapy: Reasons Which Need to Be Discussed Meticulously A good treatment should not ask, “How much cartilage is left? It must inquire, for example: “What aspects of the knee joint (or whole organ metaphors) are biologically active, inflamed, overloaded or still responding to preservation?
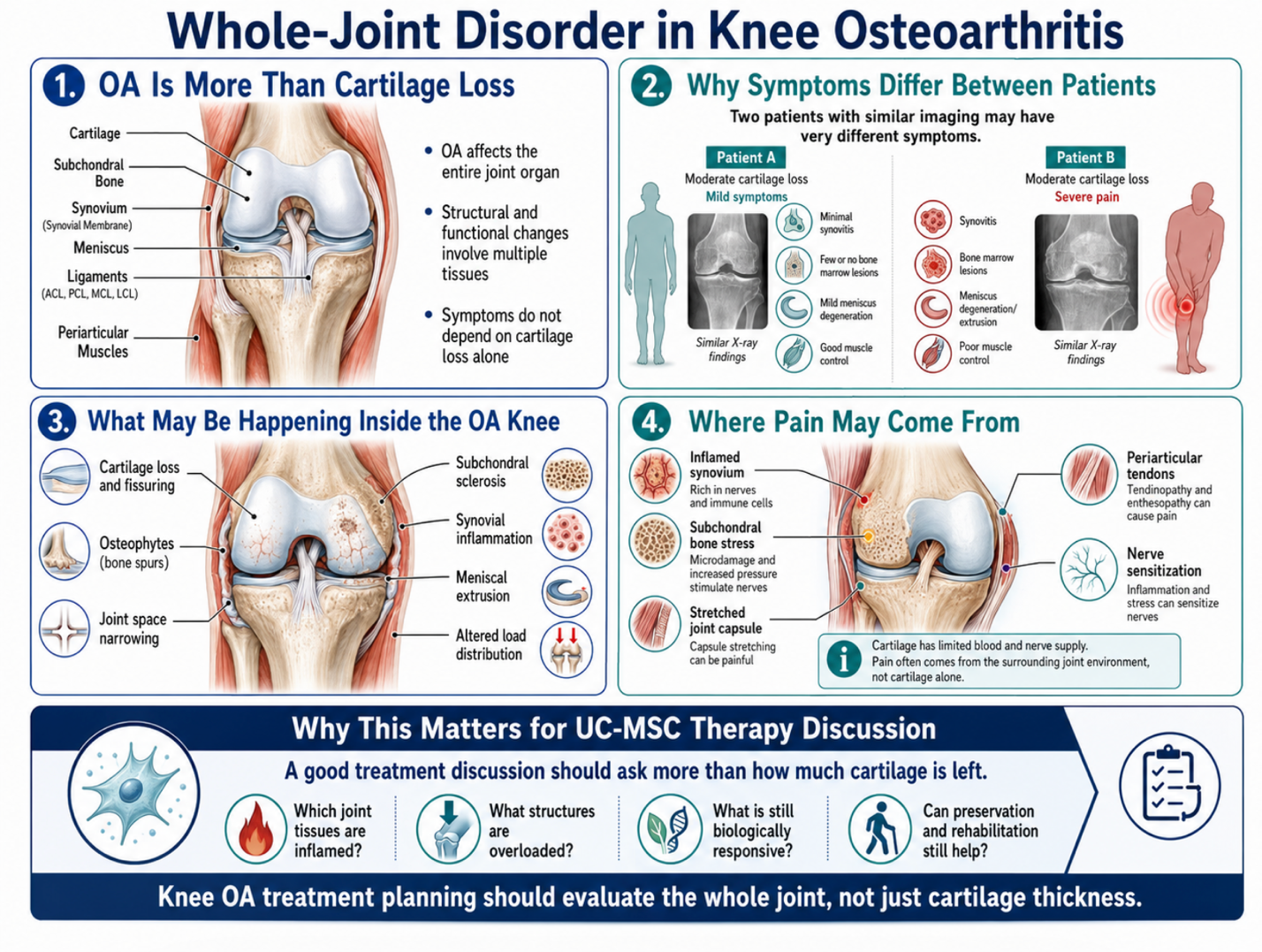
Figure 1: Structural, Inflammatory, and Mechanical Factors in Knee Osteoarthritis
Why Standard Treatment May Not Work for All Patients
Conventional knee osteoarthritis care remains key. Rehabilitation of bracing, gait correction, injections and other appropriate medication may be the conservative modality management with orthopedic review! Surgery could be justified when pain and functional limitation are advanced, and this is coupled with high-grade structural degeneration.
Yet most of the so-called standard treatments aim the symptoms or mechanics not the tissue biology. Analgesic will alleviate pain but it did not restore joint homeostasis. While steroid injections may relieve inflammation in the short-term, their repeated use must be undertaken with caution. In selected cases, response to hyaluronic acid support may be beneficial (but differs). Though important for strength and movement control, PT has not shown to fully improve synovial inflammation or cartilage-catabolic signaling.
It is exactly this gap that renders regenerative orthopedics clinically interesting. The knee injections of UC-MSC stem cell therapy are not intended to be a complete replacement for all conventional treatment. They are best viewed as a biological augmentation technique for targeted patients who have sufficient joint structural integrity to respond.
What Are UC-MSC Stem Cell Therapy?
UC-MSCs are mesenchymal stem (or stromal) cells derived from Whartonʹs jelly of the umbilical cord. That tissue is obtained from healthy birth donation and its processing is done under stringent laboratory settings. UC-MSC stem cell therapy is one of the regenerative medicinal cells that are mostly utilized and known for their paracrine properties. That means that their ability to be effective is less about being cartilage and more about the signals they release.
Such signals can comprise of cytokines, growth factors, chemokines, microRNAs, extracellular vesicles and immune-regulatory proteins. These signals may interact with synovial cells, chondrocytes, immune cells, endothelial cells and fibroblast-like cells in damaged tissue environments of the knee joint.
And this is why you should be perhaps careful with the expression “stem cell cartilage regeneration. The accurate concept is microenvironment modulation. Clustering of UC-MSCs stem cell therapy may serve to change the osteoarthritic knee away from a state persistent inflammatory and catabolic signaling toward a more repair-supportive environment.
The Resources UC-MSC Knee Injections Could Provide for Osteoarthritis
1. Synovial Inflammation Modulation
In many osteoarthritis patients, synovial inflammation is an important contributing factor in pain generation. A synovium that is inflamed can release cytokines and enzymes which not only stimulates cartilage destruction but also increases pain sensitivity. UC-MSC stem cell therapy may modulate immune-cell function and secretion of inflammatory mediators. You don’t want to turn off all inflammation, you just want to shut off the over abundance of inflammatory signaling that’s keeping the joint inflamed.
2. Cartilage-Cell Stress Support
Chondrocytes are the cells that maintain cartilage matrix. Chondrocytes in osteoarthritis: stressed, senescent or catabolic? Rather than preserving matrix, they may participate in tissue destruction. Signals from UC-MSC stem cell therapy may sustain chondrocyte survival pathways and modulate the balance dynamics associated with matrix degradation (MMPs) versus repair signaling.
This does not mean that the therapy can recreate a normal cartilage surface in late stages with any consistency. The more attainable target is to preserve the cartilage that remains, and remove the biological factors that increase degeneration.
3. Extracellular Matrix Balance
Cartilage is dependent on components of the ECM including type II collagen, aggrecan and proteoglycans. In OA, matrix-degrading enzymes may gain the upper hand over matrix-building. UC-MSC therapy is investigated owing to the possible interplay between MSC-derived factors and matrix turnover/catabolic enzyme activity.
4. Subchondral Bone and Joint Crosstalk
There is a close interaction between cartilage and subchondral bone. Once cartilage begins to thin, subchondral bone bears more load and can become thickened, inflamed or painful. Affecting Pain and disease progression Bone marrow lesions and subchondral remodeling. Thus, a regenerative paradigm should consider the unit of cartilage and bone, that is osteochondral unit rather than just cartilage.
5. Rehabilitation Tolerance
Pain limits movement. Because patients often avoid movement, quadriceps weakness, poor hip control, stiffness and weight gain can all lead to increased knee loading. If UC-MSC stem cell therapy alleviates pain and inflammatory burden in select patients, it may render them more amenable to rehabilitation. And this is important because long-term joint preservation largely relies on strengthening, movement correction, and progressive loading.
What Current Evidence Suggests
While clinical evidence supporting MSC stem cell therapy in knee osteoarthritis is still scattered, it has recently grown. Prolonged treatment data at 12 months reported by a 2024 systematic review and network meta-analysis compared the effect of advanced MSC therapy vs placebo or viscosupplementation on pain, adverse events, and quality of life as outcomes related to musculoskeletal-system-related disorders: lower pain (no difference on adverse events; uncertain certainty of evidence).
Intra-Articular MSC Injection Alone Improves Knee Pain and Dysfunction in Unoperated Knee Osteoarthritis in Patients A 2025 systematic review and meta-analysis of randomized controlled trials reported that intra-articular MSC injection alone could improve knee pain and dysfunction. Positive results must therefore still be interpreted with caution as study design differed with respect to source(s) of cultured cells, dose, processing technique before transplantation(∗), route of administration (ortho or systemic), clinical severity at baseline, follow-up period and outcome measurement.
It is easy to land at the intelligent position of “stem cells do not work” or, worse yet, “Stem Cells regrow cartilage. More realistically, MSC stem cell therapy is an evolving area with positive signals but will require appropriate patient selection and control of treatment quality, validated experimental protocols including standardized dose/method/time points for administration and appropriately evaluated short/long term outcomes.
Who could be a better candidate?
Patients with mild-to-moderate knee osteoarthritis, persistent pain despite conservative treatment methods or the following conditions should consider UC-MSC stem cell therapy knee injections:
● Recurrent synovial inflammation due to immune-mediated processes
● Early cartilage degeneration
● Ideal patients who wish to preserve their joints Pre-op patient
Biological injection alone may be less effective in patients with severe bone-on-bone arthritis, significant deformity or malalignment, large unstable meniscus tear, substantial ligament instability and active infection or inflammatory arthritis flare in the setting of advanced loss of joint space. In such cases, bigger surgery like orthopedic or joint replacement could be the better option.
A complete evaluation should include assessments of pain pattern (effect on daily activity), X-ray grade, MRI findings (where available), swelling, range of motion, alignment, walking tolerance history, previous treatments and medications used, body weight and activities sports goals pursued by the patient as well as rehabilitation history. High quality regenerative medicine starts with diagnosis, not selling an injection.
Why Local Injection Planning is Important
Intra-articular injection is commonly talked about for knee osteoarthritis as this is the main joint of interest. Through local delivery, the MSC stem cell therapy deliver biologics in the local area of synovial fluid, at the cartilage surface, in contact with the synovium and within that joint environment. Sometimes ultrasound guidance is required to improve accuracy in inaccessible / oedematous regions.
A knee injection, however, is not always sufficient. In the presence of poor quadriceps strength, obesity, varus alignment, unstable meniscus damage, or poor gait mechanics there will still be damaging mechanical signals received by the joint. Biology and biomechanics must be analysis together.
Therefore, a comprehensive and effective UC-MSC stem cell therapy knee program should include rehabilitation guidance (not just cell delivery).
Safety and quality control, cell information
In UC-MSC stem cell therapy, product quality is at the heart of issue. Key safety aspects concern the donor screening, testing for infectious diseases (Bethall et al. 2012), sterility testing (Ahrens et al. 2007; Le Blanc and Ringdén 2009) and endotoxin testing (Fischer et al. 2010), as well as cell identity markers, viability and culture conditions at transport time, followed by the administration by a physician (Bensinger et al. 1988).
It is not just how many cells there are, though. An inadequate viability, inadequate documentation after exposure to cryo-destructive temperatures, high-contamination risk, poor injection and/or patient selection cannot be compensated by a high dose. More important is to ask, Are the cells well characterized, fresh, living (viable), sterile and suited for the condition of the patient?
Just as regulatory claims should not be too sanguine. The FDA warns that regenerative medicine therapies are not approved in the United States to “treat orthopedic conditions, including osteoarthritis, tendonitis, disc disease, hip pain knee pain neck pain or shoulder pain.” This criticism depends on the country, as regulations do indeed vary (you’ll see this in my next point), but still serves to justify the need for transparent communication backed by evidence.
What To Expect Following A UC-MSC Stem Cell Therapy Knee Injection?
The treatment of UC-MSC stem cell therapy should not be viewed as knee reconstruction in a day. Osteoarthritis progresses over the course of years, and the structure of disease within a joint is not likely to change overnight. Gaining more realistic goals may include less pain, reduced stiffness and improved walking tolerance/function, decreased swelling frequency and volume and better compliance with rehabilitation.
So, we must look at progress with tangible results: pain score, WOMAC score, stair ability, walking distance, and ROM (range of motion), need for swabs or medication and need for analgesics/medication/sleep post-underactive return to activity, follow up imaging if clinically indicated.
Some patients may improve meaningfully. Some may respond minimally due to irreversible changes of the joint, persistent local mechanical overload or inflammation mediated by a different disease process. Honest follow-up trumps before-and-after exaggerations.
Conclusion
UC-MSC stem cell therapy knee injections are not a magic bullet that works for everyone but should be offered as an individualized treatment option to select patients with knee pain due to osteoarthritis. Knee osteoarthritis is a common degenerative joint disease of the entire joint, involving structures such as cartilage, synovium, subchondral bone, meniscus and ligaments as well as muscle coactivation in predisposition to pain which are also important factors that we must consider. For example: Inflammation and biomechanics. And therein lies the complexity that explains why a single injection is no substitute for diagnosis, rehab, orthopedic assessment and long-term joint management.
The rationale for the therapeutic potential of UC-MSC stem cell therapy relates to paracrine signalling, immunomodulation, support of cartilage-forming cells, balance of extracellular matrix synthesis and turnover and generation of extracellular vesicles (EV).
communication, and improvement of the joint microenvironment. Current research is encouraging but still developing, with ongoing questions about dosing, protocols, patient selection, structural outcomes, and long-term durability.
For patients considering stem cell therapy for knee osteoarthritis in Thailand, the smartest approach is not to chase the most dramatic promise. It is to choose careful diagnosis, high-quality UC-MSC preparation, transparent safety testing, physician-led injection, realistic expectations, and a structured rehabilitation plan.
Responsible regenerative orthopedics is not about claiming to create a new knee. It is about supporting the biology of a damaged joint while protecting the patient from unnecessary delay when surgery or other standard care is more appropriate.
FAQ
Can UC-MSC knee injections cure osteoarthritis?
No. UC-MSC knee injections should not be described as a cure. They may support inflammation regulation and joint microenvironment repair in selected patients, but results vary by disease severity, alignment, cartilage condition, and rehabilitation.
Can stem cells regrow knee cartilage?
UC-MSCs may support cartilage-related repair signaling, but they should not be marketed as guaranteed cartilage regrowth. Structural cartilage regeneration remains difficult and is still under clinical investigation.
Who may be suitable for UC-MSC knee injections?
Selected patients with mild-to-moderate osteoarthritis, persistent pain, synovial inflammation, early cartilage degeneration, and a joint preservation goal may be considered after physician evaluation.
Who may not be suitable?
Patients with severe bone-on-bone arthritis, major deformity, active infection, severe instability, large untreated meniscus tears, or urgent surgical indications may need a different treatment pathway.
Do patients still need physiotherapy?
Yes. Physiotherapy remains important. Muscle strength, weight control, gait mechanics, hip stability, and progressive loading are essential for long-term knee function.