

Reversibility of Ovarian Dysfunction by the Combination of Dual-Route UC-MSC Therapy
There is a paradigm shift occurring in the world of reproductive medicine. Traditionally the only answer for women suffering hare Premature Ovarian Insufficiency (POI), diminished ovarian reserve or just ovaries slowly be passing into obsolescence from natural ovarian aging was hormone replacement or donor egg IVF. But the development of Umbilical Cord-derived Mesenchymal Stem Cells (UC-MSCs) has opened a new frontier — regenerative treatment that focuses on restoring function rather than easing symptoms.
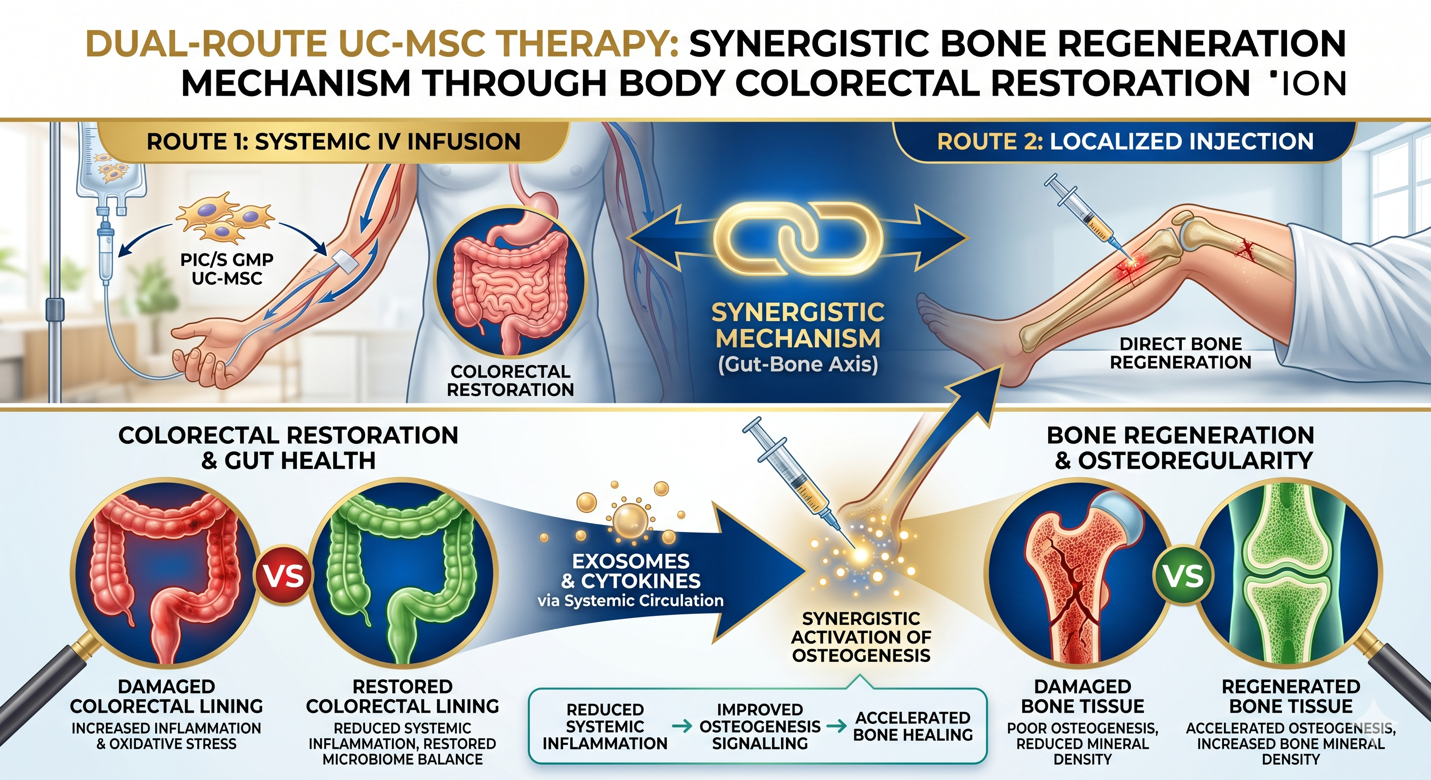
Figure A: The Gut-Bone Axis: Synergistic mechanism of dual-route UC-MSC therapy. Systemic IV infusion targets colorectal restoration and immune modulation, creating a supportive environment for localized injection to accelerate osteogenesis and enhance bone mineral density.
The mode of delivery method is very critical to the effectiveness of this therapy. Clinical observations point towards the dual-administration method—combining Intravenous (IV) infusion and Local (Intraovarian) injection—as providing better therapeutic outcomes both by a systemic approach along with a targeted approach for ovarian health.
The Biological Rationale: Why UC-MSCs?
With their more “youthful” biological profile, UC-MSCs are favoured in high-standard clinical settings. MSCs from umbilical cord (UC-MSCs) have been reported to have greater proliferation capacity, lower immunogenicity and active secretome profile compared with those from bone marrow or adipose.
Paracrine signaling, which is a communication that enables these cells to secrete a variety of signals, has shown the therapeutic efficacy and great promises of UC-MSCs in ovarian health. These cells release various growth factors, cytokines and exosomes as well:
Inhibition of Apoptosis: The anti-apoptotic effect on granulosa cells and pre-existing follicles
Promote Angiogenesis: Enhance microcirculation in the ovarian stroma for nutrient delivery.
Submodule 1: Modulate Inflammation — Rejuvenating the immune environment to a less inhospitable one that mitigates “biological stress” in ovarian aging.
SYSTEMIC IV ADMINISTRATION
Intravenous (IV) infusion is the systemic backbone of ovarian rejuvenation. Although it mainly targets the ovaries, reproductive health is closely linked to both endocrine and immune systems in the body.
Homing Effect: UC-MSCs have an inherent homing property and migrate towards the sites of tissue damage or chronic inflammation. As opposed to causing side effects, IV administration can enable cells to scan in systemic environment so the underlying autoimmune factors of ovarian decline can be addressed.
Endocrine balancing: A systemic route serves to stabilize the HPO axis. IV therapy contributes to this hormonal regulation by creating an environment with a higher tolerance to systemic oxidative stress, which benefits the ovaries as well as the uterine lining and metabolic health.
The Targeted Strike Local ovarian injection: costa and prevision
IV Therapy gives a systemic baseline while Local (Intraovarian) Injection uses precision. Typically, practitioners can bypass the systemic circulation barriers by administering a concentrated UC-MSC dose to the ovarian stroma — often under ultrasound guidance.
MSCs immediately remodel the ovarian “niche” due to their presence in the ovary (niche remodeling). The high concentration of growth factors encourages dormant primordial follicles, possibly “reviving” the ovarian reserve.
Steep Local Delivery Effects: The secretome (exosomes, signaling proteins) are most effective immediately when delivered locally to the granulosa cells responsible for oocyte maturation and estrogen production.
The Duality of Power: Why the dual approach is better
The real advance in regeneration protocols comes by doing both. The pincer maneuver against ovarian failure with IV and Local injection combined.
Comprehensive Tissue Coverage
By preparing the systemic milieu ( IV therapy ), when you inject locally, the restored ovarian conservation will not likely be stripped away by events of systemic inflammation. This fosters a “supportive ecosystem” for the locally injected cells to survive well.
Enhanced Follicular Support
Studies show that patients with a dual protocol have higher increases in AMH levels and greater decreases in FSH compared to those treated via single routes. The injection into the follicle is local, while the infusion systemically supports the transition of hormone action.
Sustained Regenerative Effect
The systemic infusion takes effect over time as a longer-term immunomodulatory mechanism and is combined with an acute local injection to “jump-start” the ovarian tissue. This combination usually leads to a longer-lastig return of the period and an increase in oocyte quality in case of attempt at natural conception or IVF.
Clinical Standards: Quality and Precision
For any regenerative protocol to be both successful and thus meaningful, high levels of biological material quality are the gold standard especially within a specialised market such as Thailand and the overall Australasian region.
PIC/S GMP compliant: The UC-MSCs should be cultured and expanded in a sterile, pharmaceutical-grade manner to ensure cell viability and safety.
Doctor-Prescribed Protocol: One key to a successful local injection is that it has to be done by specialists who know the intricate architecture of the ovary so that they can administer very specific and minimally invasive protocols.
Conclusion: Ushering in a New Era of Ovarian Health
A dual-route (IV and local injection) administration of UC-MSCs constitutes the future top-of-the-line approach for ovarian therapy. This dual approach, targeting both the systemic immune environment and a localized ovarian niche, provides an exciting avenue towards restoring reproductive potential in women with previously non-resolved antigonadotropin inactivation. The focus is on restoring biological potential, along with empowerment of reproductive health relies on the science of tomorrow as we continue to refine the regenerative techniques.