

Chronic obstructive pulmonary disease (COPD) is a common chronic condition affecting adults. It is typically the result of prolonged exposure to cigarette smoke, air pollution, occupational dust and chemical fumes or other inhaled irritants. COPD is clinically relevant, as it may not only slowly limit ventilation and exercise capacity but also contribute to an increased frequency of acute exacerbations and severely impair quality of life. COPD is characterised by chronic respiratory symptoms and persistent Airflow obstruction as per the Global initiative for Chronic Obstructive Lung Disease.
The patient with COPD may complain of long-term cough, sputum developmen, wheezing, chest heaviness or discomfort, dyspnea on exertion (DOE), fatigue upon activity effort and repeating respiratory infections1-2. In late-stage sickness, even mild physical activities such as walking, bathing, dressing, or climbing stairs may cause breathlessness. However, severe exacerbations can necessitate emergency treatments, with admission to hospital and supplemental oxygen.
COPD is a chronic disease characterized by inflammation, airway remodeling, emphysema, mucus hypersecretion and impaired gas exchange thus some of the patients seek further palliative means at one stem cell clinic in Thailand. Any discussion on stem cell therapy for COPD, however, needs to be tempered with medicine. Despite significant excitement about their potential, stem cell-based approaches should not be touted as a cure or alternative to current standard pulmonary care. A more palatable stance would be that UC-MSCs should only be considered explorative and adjuvant to appropriate COPD programs when indiscriminately used under the watchful eye of a physician.
Disease Mechanisms: Understanding COPD Pathophysiology
The pathophysiology of chronic obstructive pulmonary disease( COPD) include chronic airway inflammation, small airway narrowing, alveolar/ parenchyma destruction, mucus hypersecretion, oxidative stress and impaired gas exchange. These biological changes emerge over time and differ between patients based on disease phenotype, smoking history, environmental exposure, genetic susceptibility, infection history and comorbidities.
1.1 Chronic Airway Inflammation
Evaporating ignitions may provoke epithelium cells, phagocytes, neutrophils and other inflamed body of tissues oxygen in the airways because of COPD. These cells discharge proinflammatory media, proteases reactive oxygen species and other signaling molecules that may contribute to airway tissue damage and remodeling.
Persistently higher levels of these markers are thought to cause the gradual thickening of airway walls, including narrowing of small airways, excessive mucus production and impaired airflow. This leads to the development of a number of symptoms including chronic cough, sputum production, wheezing and breathlessness.
1.2 Emphysema and Alveolar Damage
Emphysema–COPD in some patients is emphysema, where walls of the alveoli rupture and are destroyed over time. The alveoli are the little air sacs that actually facilitate oxygen exchange. If alveolar architecture is damaged, the lungs become less efficient in exchanging O2 for CO2 into or out of the blood stream.
This may lead to a decrease in exercise tolerance, lower levels of oxygen, fatigue and severe impairment of pulmonary function.
Hypersecretion of mucus is caused by inflammation in airway epithelial cells, including goblet cell hyperplasia resulting from inflammatory cytokines and exposure to chronic stimuli: (1) excessive secretion of mucus via overload or hypertrophy; the production of numerous asthma mediators such as IL-2 through cellular activation; other cytokines causing morphological changes leading to inflammation in tonic bronchial structures, which produce an asthmatic response.
Chronic bronchitis characteristics are also widespread in COPD with mucus hypersecretion, airway irritation or inflammatory signs. Excessive mucus can narrow the airways, lead to more cough, and ultimately make patients more susceptible to infections or exacerbations.
1.3 Oxidative Stress and Tissue Damage
Oxidative stress has a central role in the pathogenesis of COPD. Reactive oxygen species (ROS) derived from cigarette smoke, air pollution, inflammation and cellular stress can injure airway cells, disturb the repair response and enhance inflammation.
1.4 Exacerbations and Disease Progression
COPD exacerbation is an episode of acute deterioration which, in most cases, is powerful triggered by infection, pollution or environmental irritants. Recurrent exacerbation can further precipitate functional decline, increase the likelihood of re-hospitalizations, and adversely affect chronic disease trajectory in the long-term.
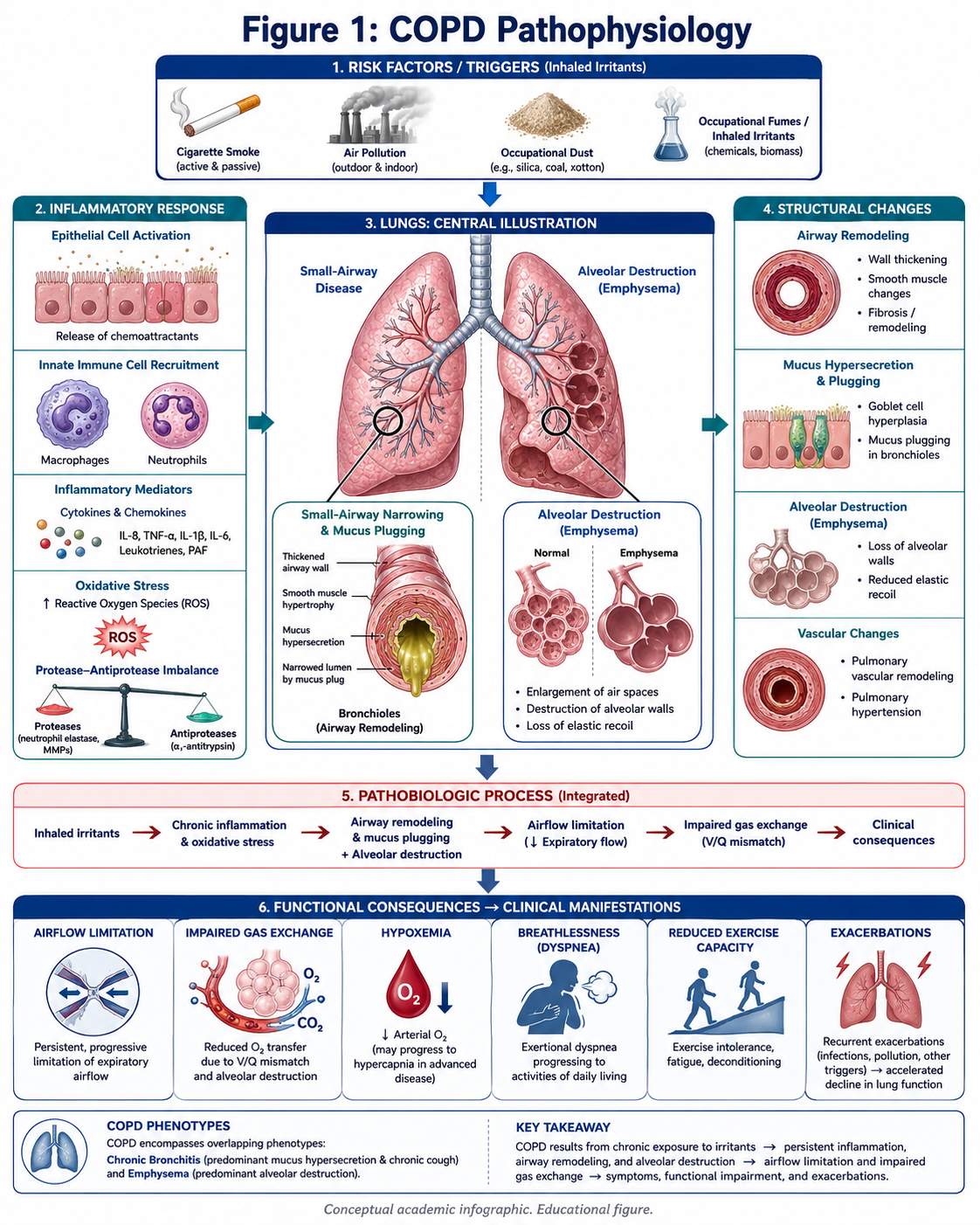
Figure 1: COPD Pathophysiology
Main mechanisms involved in chronic obstructive pulmonary disease (COPD): diffuse and chronic inflammation of small airways, which leads to airway narrowing, mucus hypersecretion and destruction of the alveolar walls; oxidative stress contributing to gas exchange impairment at rest and during exertion, leading to recurrent exacerbations.
The Limitations of Traditional Treatment for COPD
The present management of COPD is intended at minimizing symptoms, enhancing exercise tolerance, reducing exacerbations, controlling associated disorders as well as boosting quality of life. Smoking cessation, inhaled bronchodilators, inhaled corticosteroids in certain patients, vaccinations such as the seasonal influenza vaccine and pneumococcal vaccines (PCV13 and PPSV23), pulmonary rehabilitation (PR), oxygen supplementation therapy for patients with hypoxemia (> 88% SpO2 at rest), management of acute exacerbations and support for weight loss or gain are some standard care practices, with regular follow-up monitoring also recommended. According to the American Lung Association, raising money for COPD includes medicines, oxygen or pulmonary rehabilitation and supportive social help.
2.1 Bronchodilators
Bronchodilators are often used to relax smooth muscle in the airways and improve airflow. They may provide relief from breathlessness and allow people to do more activity, but will not reverse damage done to the lungs.
2.2 Inhaled Corticosteroids
Inhaled corticosteroids should be used in selected populations of COPD patients with frequent exacerbators or specific inflammatory phenotypes. While they can help lower risk of exacerbations in select patients, they unfortunately come with risks as well including pneumonia (and even death) in some instances.
2.3 Oxygen Therapy
You may also have oxygen therapy in severe COPD with low blood oxygen levels. Oxygen therapy is critical for select patients but does not restore injured alveolar tissue.
2.4 Pulmonary Rehabilitation
Pulmonary rehabilitation is an established evidence-based aspect of COPD management. Exercise training, breathing techniques, education, nutrition support and psychological or social support are often part of it. According to the American Lung Association, pulmonary rehabilitation is a supervised program that can help people with chronic lung disease breathe more easily and improves quality of life.
2.5 Limitations of Conventional Treatment
Existing COPD therapies are modestly effective in alleviating symptoms and decreasing risk of exacerbations, but do not completely reverse these long-lasting structural lung changes. This restriction has stimulated a focus on adjunctive and investigational strategies, including regenerative medicine as well as UC-MSCs for COPD.
UC-MSCs for COPD: Scientific Positioning
Hallmarks of UC-MSCs, or MSCs from the umbilical cord, include immunomodulation, anti-inflammation/immune suppression, paracrine effects and tissue support1 and make it a critical focus in regenerative medicine. The rationale for the use of UC-MSCs in COPD is derived from their involvement in various inflammatory and destructive pathways encompassing the injury to airway and alveoli.
But we did not characterize UC-MSCs as directly regenerating lungs or treating COPD. Importantly, current clinical evidence is limited and stem cell-based strategies for COPD remain clinical investigational. MSCs are administered systemically in moderate to severe COPD in a placebo-controlled randomized trial and while the MSC administration appeared safe, the study did not establish them as a curative treatment of proven effectiveness for COPD.
A medically appropriate statement is:
While much remains to be discovered, UC-MSCs could be considered an investigational adjunct treatment in select COPD patients with modulating roles in immune modulation, repair of inflammatory balance, and oxidative stress as well as paracrine signaling.
Speculated Mechanisms of UC-MSCs in COPD Support
4.1 Immunomodulatory Signaling
In COPD there is a chronic activation of inflammatory pathways. However, UC-MSCs appeared to be released multiple signaling molecules and their potential interaction with immune cells such as macrophages, neutrophils, T cells or epithelial cells. This could theoretically support a more favorable inflammatory environment.
4.2 Anti-Inflammatory Communication
UC-MSC Therapy are frequently investigated for their propensity to secrete a broad range of cytokines, growth factors, extracellular vesicles, and other paracrine factors. Signals of the signalling may modulate inflammatory communication and tissue stress responses.
4.3 Support for Tissue Microenvironment
For example, oxidative stress and inflammatory mediators might impinge on the lung microenvironment in COPD with impaired repair signaling and endothelial dysfunction. Through cell signaling, UC-MSCs may potentially be involved in augmenting the tissue environment more favorably.
4.4 Paracrine and extracellular vesicle activity
The role of UC-MSCs may be more strongly related to paracrine effects than with direct cell replacement. Research on the same has revealed UC-MSC-derived signaling molecules and extracellular vesicles as potential effector mediators of cell communication, immune regulation, and tissue-supportive pathways.
4.5 Important Limitation
The proposed mechanisms are science-friendly but do not confirm any clinical benefit. Stem cell clinics in Thailand conducting such COPD related programs should always make clear that UC-MSCs are a investigational and supportive treatment option and an established cure.
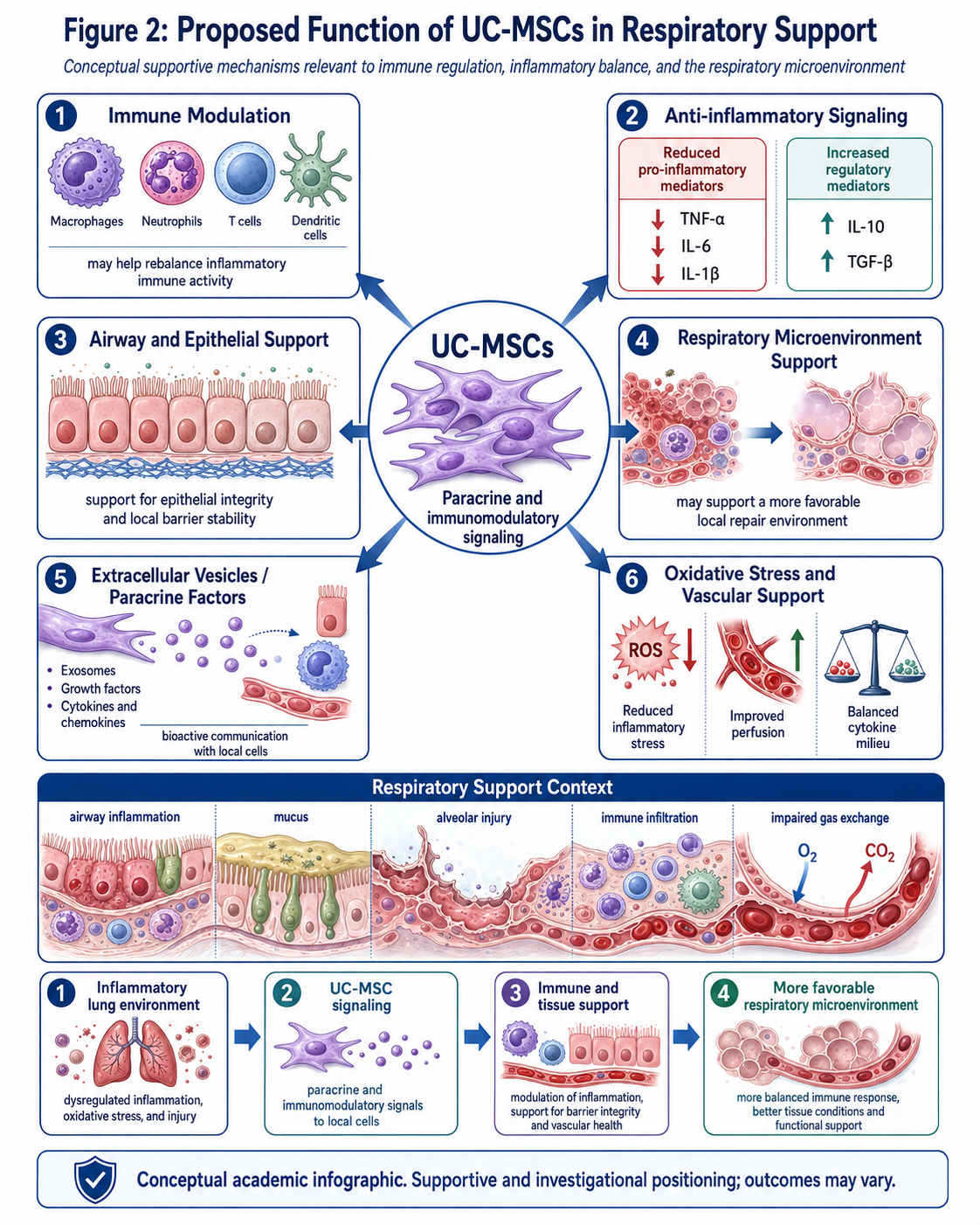
Figure 2: Proposed function of UC-MSCs in respiratory support
Support role of UC-MSCs in COPD
The figure summarizes proposed mechanisms by which UC-MSCs may support COPD, including immunomodulatory signaling (blue), anti-inflammatory communication (pink), paracrine activity (green), release of extracellular vesicles; regulation of oxidative stress state; and amelioration strategies that help provide a more appropriate lung microenvironment.
COPD: How to Find a Stem Cell Clinic in Thailand
Thailand is well known for international medicine, wellness and privatized health care. Thailand provides medical coordination, international patient support, rehabilitation programs and regenerative medicine for patients looking for a stem cell therapy clinic for COPD.
Selective Reverse Clinical TrialHowever, you must well selection in clinics. As COPD is a life-threatening respiratory disease, any regenerative strategy should be combined with the standard of pulmonary care rather than replace it.
Closing
Patients looking for stem cell clinic in Thailand for COPD should not simply look for a stem cell clinic offering UC-MSCs but rather one that offers them as part of a medically-supervised, transparent, realistic and integrative program with conventional respiratory care. Chronic immune airway inflammation, emphysema, mucus hypersecretion and air trapping, oxidative stress to lung parenchyma and intravascular space driving impaired gas exchangeand recurrent exacerbations combine to morph this complex into COPD. Conventional treatment continues to play a role in controlling symptoms and preventing relapse.
However, their properties of immunomodulation/anti-inflammatory, paracrine and tissue-supportive signaling structures may offer a potential supportive/investigative developmental approach in selected COPD patients. But they also must not be viewed or marketed as a substitute of pulmonologist-recommended therapies. An evidence-based approach for COPD in Thailand must be based on prudent regenerative medicine responsible positioning with simultaneous pulmonary rehabilitation and supervised monitoring through realistic expectations.