Systemic lupus erythematosus, or SLE, is a complex systemic autoimmune disease in which the immune system falsely attacks healthy tissues in the body. It may involve the skin, joints, kidneys and blood vessels as well as the nervous system and other organs of the body. According to available evidence/discussion, normal treatment remains crucial including corticosteroids, immunosuppressive mediation, biologics, and cautious expert follow-up. With half of the patients still receiving systemic glucocorticoids 5 years after diagnosis, EULAR recommendations now focus on achieving disease control, avoiding flares and organ damage and minimizing longterm glucocorticoid exposure if appropriate.
The interest in DFPP and Stem cell therapy for SLE is a newer, supportive immune-based strategy. The idea here is not to replace routine lupus care but rather how enhanced blood purification and regenerative cell signalling may improve the internal immune milieu of select patients.
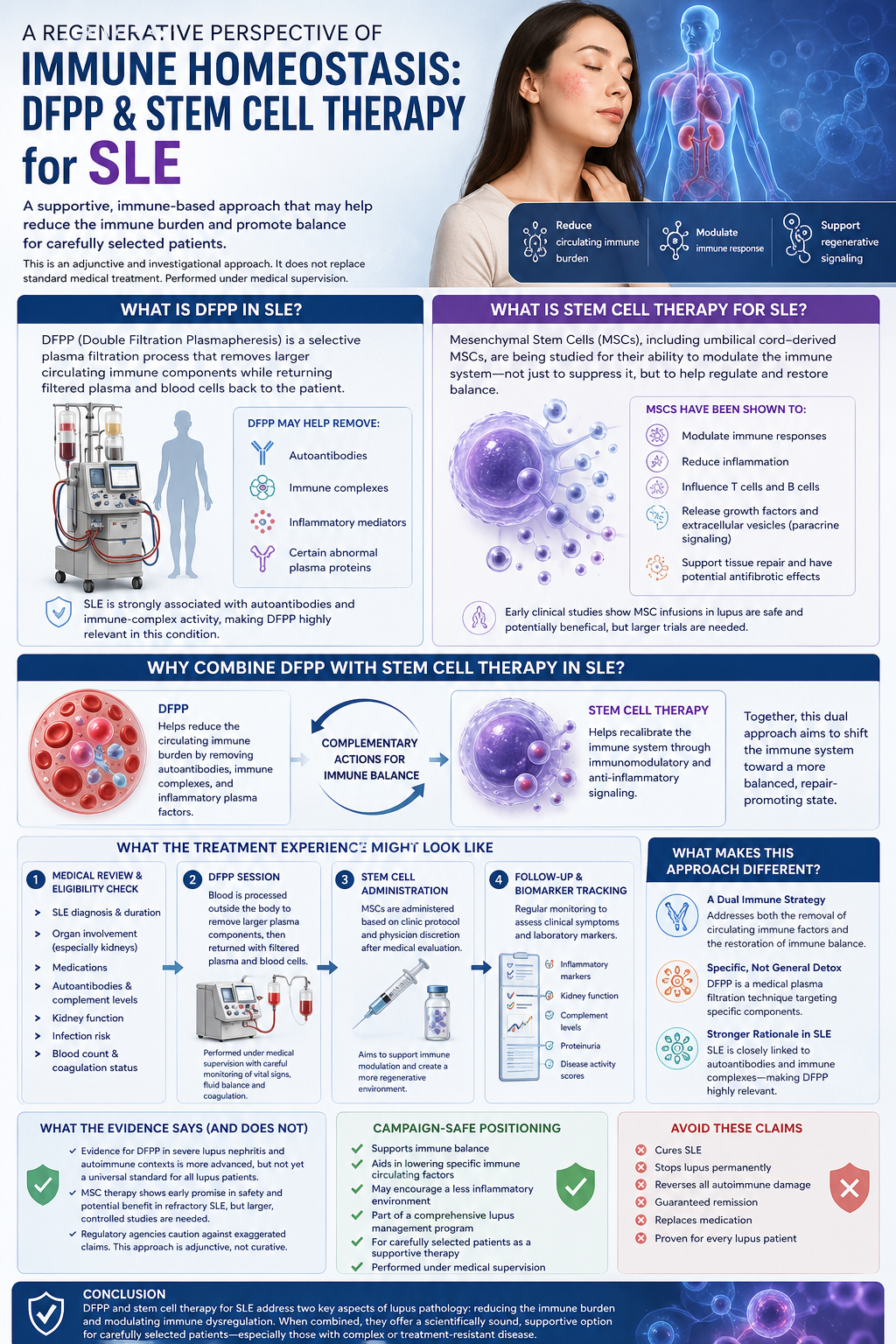
What Is DFPP in SLE?
Plasmapheresis is a selective plasma filtration process for DFPP. In a treatment, blood is taken from the patient, plasma separated off from the blood cells and run through a second filter that removes larger circulating components.
In SLE, these may include:
Autoantibodies
Immune complexes
Inflammatory mediators
Certain abnormal plasma proteins
This is important because of the strong association between SLE with autoantibody production and immune-complex mediated activity. In other words, DFPP has a stronger disease-specific rationale in SLE than it does in many of the other conditions where it has been applied. Severe lupus nephritis (2024 study) Description: A 2024 study from our group reported that immunosuppressive agents with or without concurrent doses of DFPP were evaluated as adjuncts to plasma exchange-based treatment strategies for conversion to remission of severe lupus nephritis.
Back What Is Stem Cell Therapy for Systemic Lupus Erythematosus?
Stem cell therapy in SLE ultimately refers to mesenchymal stromal/ stem (MSCs), including umbilical-derived MSCs. Importantly, they are not being investigated as a means of immune suppression, albeit that MSCs have been shown to suppress immunity but it was now realized that they may play the role of regulators (Moraes et al. 2013).
MSCs have been characterized as:
Immunomodulatory effects
Anti-inflammatory signaling
Impact on T cells and B cells
E (paracrine) signaling by growth factors and/or exocytic release of extracellular vesicles
Possible antifibrotic and tissue-supportive properties
That study, a phase 1 trial of umbilical cord MSC infusions in lupus, indicated the infusions were highly safe and possibly efficacious—yet larger trials are needed.
SLE: The Rationale for Combining DFPP and Stem Cell Therapy Why Would You Combine DFPP with Stem Cell Therapy?
In support of SLEs, the rationale for combining DFPP and stem cell therapy is two-fold due to complementary actions.
DFPP may decrease the circulating immune burden by decreasing autoantibodies, immune complexes and inflammatory plasma factors. Mononuclear cells may then assist immune recalibration via immunomodulatory and anti-inflammatory signaling as co-treatment with stem cell therapy.
A simple way to explain it:
It allows for the removal of certain selected inflammatory and antibody-related factors from the blood (DFPP) Perhaps stem cells could be utilized to drive the immune system into a more balanced repair-promoting state.
Despite this combined approach, it is still best characterized as adjunctive and investigational rather than curative. But that’s because the biological rationale is sound, since SLE has both circulating immune factors and deeper immune-system dysregulation.
What the Treatment Experience Might Look Like
Stages of a medically supervised DFPP and stem cell program for SLE may include:
Medical Review and Eligibility Check
A complete medical assessment is the first step with this patient. This may include review of:
SLE diagnosis and disease duration
Organ involvement, especially kidney involvement
Current medications
Autoantibody profile
Complement levels
Kidney function
Infection risk
Blood count and coagulation status
DFPP Session
Blood going through a process outside the body during a DFPP session The objective is to selectively eliminate larger plasma components whilst returning filtered plasma, along with blood cells, back to the patient.
Usually, the session is under medical supervision and followed by blood pressure, vascular access, fluid balance and safety in terms of coagulation mechanism.
Stem Cell Administration
MSCs may be administered based on both clinic protocol and physician discretion after medical evaluation. Its aim is direct organ replacement or even immune modulation and biological support.
Follow-Up and Biomarker Tracking
Follow-up may involve clinical symptom review as well as laboratory monitoring including inflammatory markers, kidney function, complement levels, proteinuria and disease activity scores where appropriate.
What Makes This Approach Different?
A Dual Immune Strategy
Most of the treatments seek to either suppress immune activity or control symptoms. This two-part concept is based on the initial use of DFPP plus stem cell therapy to reduce circulating immune burden, and subsequently administering chronic stem cells over a prolonged time to promote immune modulation via regenerative signaling.
Specific Detox Claims Rather than General
DFPP is NOT a nebulous “detox.” This is a medical plasma filtration based method to reduce selected plasma components. It bolsters the scientific cred of the campaign.
Stronger Rationale in SLE
SLE has a more evident link between circulating autoantibodies and immune complexes than with some neurological conditions. This makes DFPP more easily scientifically communicable in a SLE campaign.
What The Evidence Says And What It Does Not
In severe lupus nephritis and autoimmune contexts, evidence for DFPP in SLE is relatively more advanced than many other diseases yet it still does not meet the bar to be adopted as a universal standard among all lupus patients. MSC therapy also shows early promise when it comes to safety signals and potential clinical benefit in refractory SLE, however the reviews continue to highlight the need for more robust, larger controlled studies.
FDA also cautions that many regenerative medicine products are advertised with claim language that exceeds what has been evaluated for safety, purity, potency or effectiveness to the extent where it avoids treatment-oriented content such as cure language and guarantee claims.
Campaign-Safe Positioning
Use phrases like:
Supports immune balance
Aids in lowering specific immune circulating factors
They may encourage a less inflammatory environment
Created in the context of a comprehensive lupus management program
For carefully selected patients, a regenerative approach is a reasonable supportive treatment.
Performed under medical supervision
Avoid:
Cures SLE
Stops lupus permanently
Reverses all autoimmune damage
Guaranteed remission
Replaces medication
Proven for every lupus patient
Conclusion
DFPP and stem cell therapy for SLE are scientifically intriguing because they address two central aspects of lupus pathology, namely, persistent immune burden and immune dysregulation. The reduction of autoantibodies selected as well as immune complexes and inflammatory plasma factors may be assisted by DFPP while MSC-based therapy can promote immune modulation due to paracrine and anti-inflammatory signaling.
A responsible rendering of this topic is a medically-monitored, supportive, and experimental treatment for carefully selected patients—particularly those with complicated or hard-to-treat disease—not as an absolute cure. Striking this balance makes the campaign sound sophisticated, believable, and high end whilst also being scientifically prudent.