

Stem Cell Therapy Thailand and Ovarian Function: What Stem Cell IVF Research Really Shows
Why this topic keeps drawing attention
This is because people searching stem cell therapy Thailand for ovarian issues generally are not looking for physics. The world of fertility is filled with tales of hope and heartache, women searching for a way forward through diminished ovarian reserve, premature ovarian insufficiency (POI), multiple failed IVF cycles, or simply the dread that time has passed them by. That’s the emotional gravity that makes this a subject that needs to be tread carefully. This is also real research, but really easy to reduce, in an oversimplified way. In practice, stem-cell IVF is a catch-all term for therapeutic strategies focusing on ovarian function (dysfunction), particularly how they may relate to the care of females with low or diminished ovarian reserve [1]. Very catchy, but not exactly a division into categories of guidelines. In cell therapy — stem-cell-based approaches in assisted reproduction, a 2025 review stressed that though this is an exciting new frontier for IVF with clinical potential, it needs meticulous and special attention by both physicians and lawmakers to ensure proof of concept under ICY certification as well as the necessity of ethical oversight (clinical validation) alongside regulatory harmonization.
Why ovarian biology comes first
Ovarian reserve is not the same thing as fertility
Before any regenerative discussion, it helps to get the language right. ASRM defines ovarian reserve as the number of oocytes remaining in the ovary. Markers such as AMH and antral follicle count can help predict oocyte yield after controlled ovarian stimulation, but ASRM is equally clear that these markers are poor independent predictors of reproductive potential. That distinction matters more than most articles admit. A better number on paper is not automatically the same thing as a better pregnancy outcome.
Ovarian aging is both quantitative and qualitative
A recent ovarian aging review article describes it as deterioration of both follicle number and quality, influenced by oxidative stress, hormonal changes, mitochondrial dysfunction, and alterations in the ovarian microenvironment. This does help to explain ovarian regenerative medicine, capturing almost all of the excitement: it is not just about fewer follicles but also a reduced supportive tissue microenvironment. To put it in another way, ovarian ageing is far from just depletion. It is altered biology.
Where stem cells enter the ovarian conversation
The main targets are POI and poor ovarian response
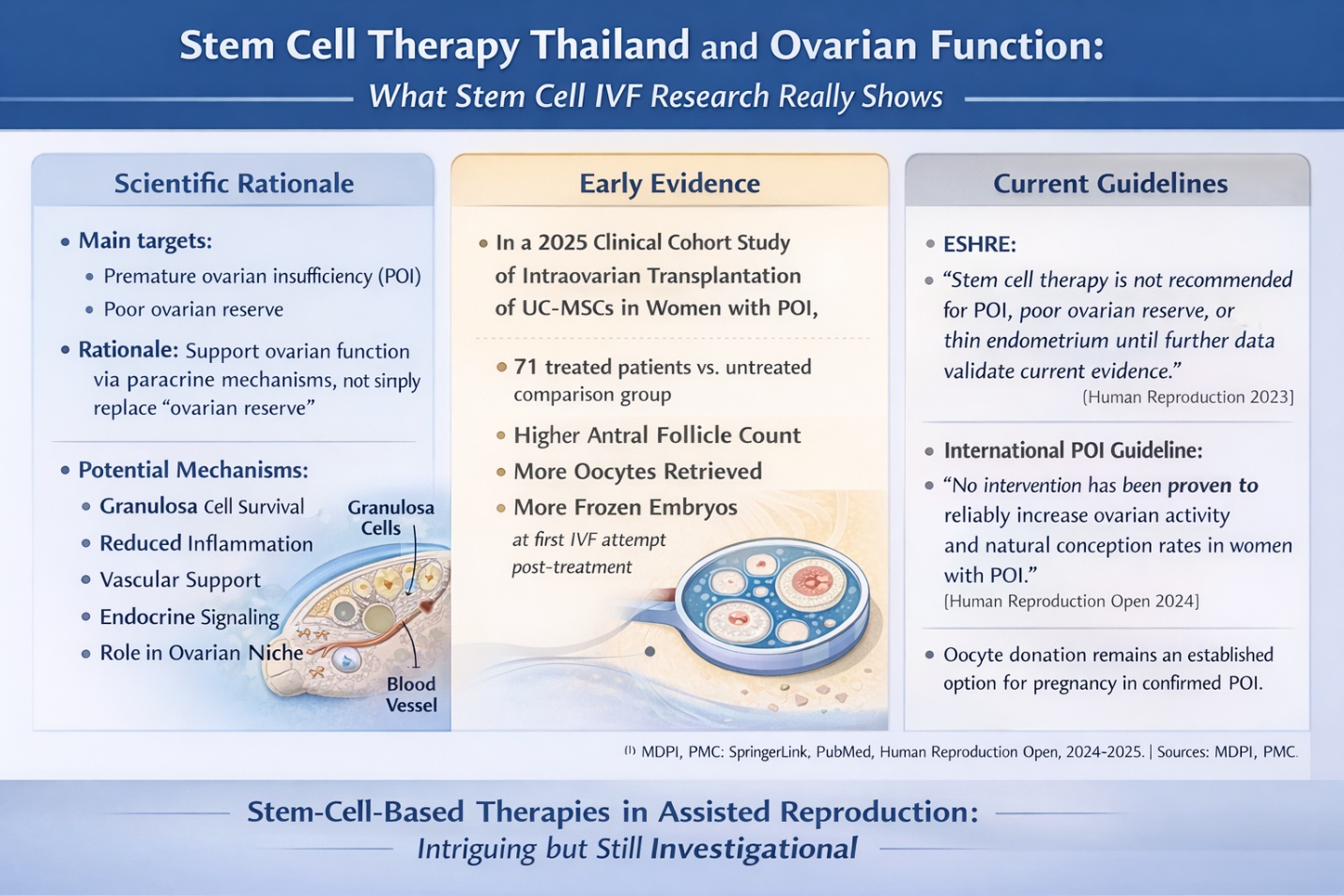
Most serious stem-cell work in this area focuses on women with premature ovarian insufficiency or diminished/poor ovarian reserve, especially when conventional IVF outcomes are limited. The 2024 international POI guideline states that POI substantially reduces the chance of natural conception, although intermittent ovarian activity can still occur in some nonsurgical cases. The same guideline also says that, for women with POI, there are no interventions that have been reliably shown to increase ovarian activity and natural conception rates, while oocyte donation remains an established option to achieve pregnancy. That is the backdrop against which stem cell IVF is being explored.
Why stem cells are being studied at all
It is not difficult to understand the scientific rationale. Stem-cell-based approaches, largely acting through paracrine mechanisms rather than merely replacing ovarian tissue, but with direct or indirect effects on granulosa cell survival pathways, inflammation, vascular support, endocrine signaling, and the wider ovarian niche have been studied. This literature review published on ovarian aging and mesenchymal stem cells in 2025 classified these therapies as a basis for slowing down age-associated alterations within the ovary that may enhance subsequent folliculogenesis from such oocytes, particularly wherein non-clinical and early-stage translation medical application are recognized to be fruitful.
What the evidence actually shows in IVF-related settings
There are early human signals, but they are still early
One of the more discussed recent studies is a 2025 clinical cohort study of intraovarian UC-MSC transplantation in women with POI. The study included 71 patients and reported higher antral follicle count, more oocytes retrieved in the first stimulation cycle after treatment, and more frozen embryos in the treated group than in the comparison group. The authors described the strategy as promising, but also explicitly called for larger multicenter studies to clarify long-term safety and efficacy. That is the key point: the signal is interesting, but it is still not the same thing as established routine care.
Systematic reviews are asking the right question, not declaring victory
A systematic review published in Journal of Assisted Reproduction and Genetics, specifically designed for full assessment of effectiveness & safety, feasibility on cellular therapy targeting at POI and DOR was published post 2025, which indicates a lot about the status quo maintained till now, even after so many years. It is prominent enough to warrant a structured synthesis of evidence but not so developed as to be regarded as established practice. That balance is key with any article that uses the keyword stem cell IVF.
What the guidelines say matters most
Current guidance is more cautious than clinic language
This is the part that most readers deserve to hear clearly. ESHRE’s good practice recommendations on IVF add-ons state that stem cell therapy for premature ovarian insufficiency, diminished/poor ovarian reserve, or thin endometrium is not recommended. The document explains that the biological rationale is unclear, efficacy data are limited, most human evidence comes from small observational studies, and there are serious safety concerns. That is about as direct as a professional society can be.
IVF outcomes should not be reduced to one biomarker
This caution also fits with ASRM’s position on ovarian reserve testing. AMH and AFC can help clinicians estimate likely oocyte yield, but they do not independently predict the chance of reproductive success. So even if a stem-cell-based intervention appears to improve AFC or response to stimulation, that still does not automatically prove better implantation, better live birth rates, or durable restoration of ovarian biology. In fertility medicine, surrogate improvement and meaningful outcome improvement are not the same thing.
How to read “stem cell therapy Thailand” claims more intelligently
Better questions usually reveal the real quality of the offer
When evaluating stem cell therapy Thailand claims around ovarian treatment, the most useful questions are not the most dramatic ones. Ask what exact diagnosis is being treated: POI, poor ovarian response, diminished ovarian reserve, or age-related ovarian decline are not identical problems. Ask what outcome is being measured: hormone values, antral follicles, oocyte yield, embryo freezing, clinical pregnancy, and live birth are not interchangeable. And ask whether the intervention is being framed as investigational or as something already proven. Good science usually sounds more careful than marketing.
The most honest conclusion
The truth is neither dismissive nor breathless. Stem-cell-based ovarian research is one of the most emotionally compelling areas in reproductive medicine because it speaks directly to loss, time, and the desire for genetically related pregnancy. There are early human signals that deserve attention, and the mechanistic rationale is real. However, there is still a more cautious stance on the current guideline position: stem-cell interventions for POI or poor ovarian reserve should not be offered as routine add-ons to NHS-funded IVF in women with POI or poor ovarian reserve, and although oocyte donation remains an established fertility option in confirmed POI, it may only provide marginal benefit. At this stage, stem cell therapy Thailand, ovarian regeneration, and stem cell IVF should be regarded as little more than serious but still experimental medicine rather than settled clinical fact.
Frequently Asked Questions
1) What does “stem cell IVF” usually mean?
Usually it refers to stem-cell-based interventions being explored around ovarian function or IVF outcomes, especially in women with POI or poor ovarian reserve. It is a common search phrase, but not a formal guideline-defined IVF treatment category.
2) Is stem cell therapy already recommended for poor ovarian reserve?
No. ESHRE’s add-ons recommendations state that stem cell therapy for POI, diminished/poor ovarian reserve, or thin endometrium is not recommended for routine use.
3) Has any study shown improvement in IVF-related outcomes?
Yes, early studies have reported signals such as higher AFC, more oocytes retrieved, and more frozen embryos after intraovarian UC-MSC treatment in selected POI patients. But those studies remain early and do not yet establish routine clinical use.
4) If AMH or AFC improves, does that prove fertility is restored?
No. ASRM states that ovarian reserve markers are useful for predicting oocyte yield, but they are poor independent predictors of reproductive potential.
5) What is the established fertility option for women with POI?
According to the 2024 international POI guideline, oocyte donation is an established option to achieve pregnancy after a diagnosis of POI.