

Diabetes is also called a blood sugar issue. We recommend monitoring glucose, lowering HbA1c, losing weight, and preventing all disease-modifying drugs and complications for the patients. All of this matters. But this is not merely a sugar vs diabetes question here. It also involves chronic inflammation, oxidative stress, fatty liver and vascular burden, insulin resistance, pancreatic beta-cell burnout, kidney predilection, deteriorating nerve structure, and metabolic strain.
This is why many patients are now searching for the best stem cell clinic and asking whether stem cell therapy for diabetes can help support the body beyond standard glucose control.
The straightforward response is: stem cell therapy will not cure diabetes, nor should it be offered as a substitute for endocrinology care, insulin or prescribed medication. Mesenchymal stem cells are increasingly studied for support of inflammation balance, tissue signaling, and regenerative biology pathways (immunological modulation) via oxidative stress pathway signals between themselves that regulate the metabolic environment in which insulin resistance exists; these MSC subtypes make UC-MSCs a minority targeted therapy.
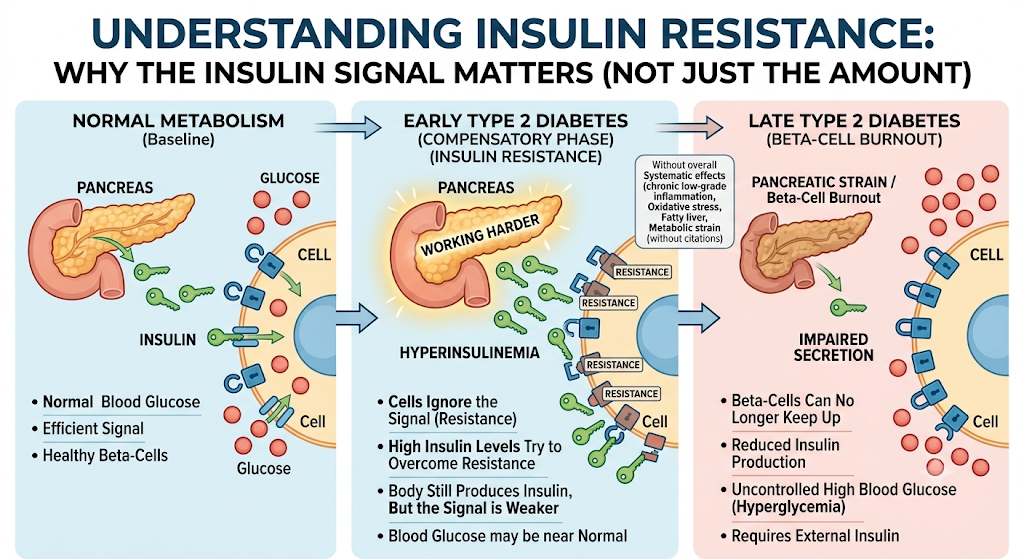
Why Insulin Resistance Is More Than High Blood Sugar
The Body Still Produces Insulin, But the Signal Is Weaker
The pancreatic insulin secretion is impaired only in the later stages of Type 2 diabetes, and may still be within normal levels at earlier points. The cells stop responding as well to insulin. This is called insulin resistance.
When this happens, the pancreas has to work harder to release more insulin. Over extended periods of time, this repeated strain may tire beta-cells out. For example, patients can begin with “high insulin,” and the pancreas’s function gradually declines.
And one reason why two patients can share the same HbA1c but have very different biology. At this level, you could have extreme insulin resistance and fatty liver. Another possibility is reduced insulin production. Another could already be exhibiting the signs of nerve damage, have issues with circulation, and even have stress on their kidney function or slow wound healing.
A less responsible clinic should not see only one HbA1c. An appropriate metabolic assessment should involve evaluation of fasting glucose, insulin, and C-peptide, HbA1c (glycosylated hemoglobin), renal function tests, hepatic function including transaminases; serum lipid levels such as triglycerides and cholesterol fractions, blood cell count, or markers for inflammation: anthropometry through body composition to determine visceral fat area or waist circumference, screening for hypertension, family history, medication review, complications evals
What Stem Cell Therapy for Diabetes Really Means
UC-MSCs Are Not Simply “New Insulin Cells”
Many people mistakenly think that diabetes stem cell therapy involves injecting cells that immediately become insulin-producing beta-cells. That’s not an appropriate way of explaining UC-MSC therapy.
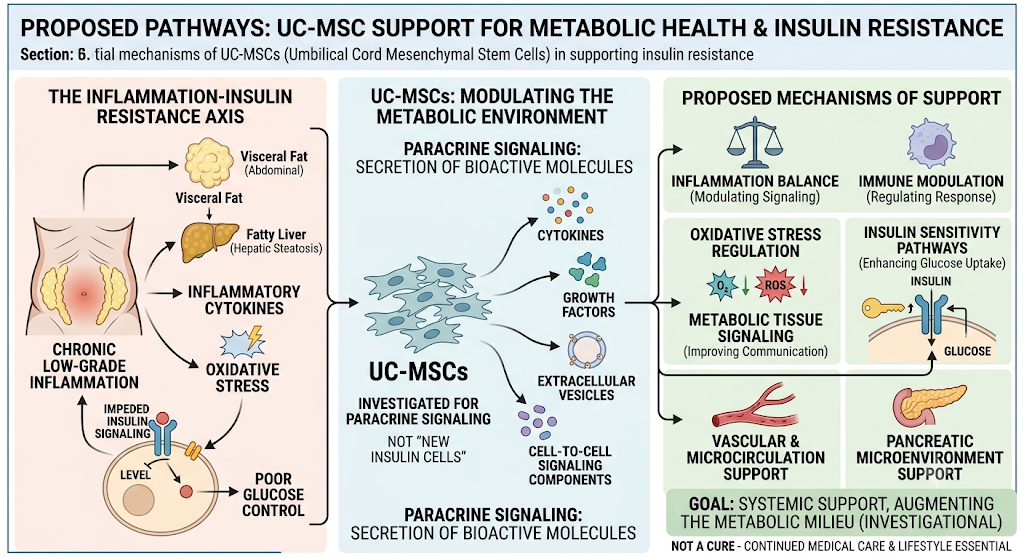
Most UC-MSCs, or those that are isolated from the placenta and umbilical cord, have the most studies for their paracrine signaling. This means that they secrete bioactive molecules such as cytokines, growth factors, extracellular vesicles, and other cell-to-cell signaling components.
In diabetes and insulin resistance, these signals are being investigated for their potential to support:
Inflammation balance
Oxidative stress regulation
Immune modulation
Vascular and microcirculation support
Pancreatic microenvironment support
Metabolic tissue signaling
Insulin sensitivity pathways
This does not mean UC-MSCs cure diabetes. It means they may support the biological environment involved in metabolic dysfunction.
Why the Best Stem Cell Clinic Should Focus on Patient Selection
Not Every Diabetes Patient Is the Same
The one thing that is constant with patients Googling about the best stem cell clinic is price or number of cells. They should query whether the clinic understands patient selection.
How you approach a patient with early insulin resistance should be different than one with long-standing diabetes, CKD, or neuropathy (vasculopathy) or very low C-peptide. The essence of conversation: A patient who retains some regenerative ability (imagine the beta-cells still fresh after a transplant) will be handled differently than an individual whose body’s own are little more than apparitions in terms of structure.
This is where C-peptide comes into play. C-peptide assists in gauging the amount of insulin still manufactured by the body. This does not provide an answer to everything, but a piece of useful information in the discussion on achievable aims for stem cell therapy approaches for diabetes.
A Good Clinic Should Not Promise Medication Discontinuation
You are tasked to ask if a responsible clinic would promise that patients could stop insulin, discontinue metformin, or reverse diabetes indefinitely after treatment and/or achieve normal HbA1c. These claims are not appropriate.
More attainable targets may include aiding in metabolic balance, decreasing the inflammatory burden, and improving tissue environment, promoting circulation and recovery pathways, as well as acting synergistically with standard medical care.
How UC-MSCs May Support Insulin Resistance
The Inflammation-Insulin Resistance Connection
Insulin resistance is associated with an ongoing low-grade inflammation state. Visceral fat and fatty liver, which have been implicated in oxidative stress as well as inflammatory cytokines can impede insulin signaling. This may, of course, render glucose control more challenging and result in complications later on.
It is possible that UC-MSCs may serve as a type of anti-inflammatory support in this context, specifically needed for modulating inflammatory signaling. You control inflammation, you favor oxidative stress and perhaps metabolic competition for insulin. However, this is a fairly new field of research and one that should be approached with care.
Why Systemic Support Matters
The mention of diabetes does not end with the pancreas. It can impact blood vessels, nerves, kidneys, skin repair, the cardiovascular system, and the eyes. That is why for diabetes, stem cell therapy often comes up in the context of systemic as opposed to single-organ support.
Not all patients may be “lower sugar now.” Perhaps a larger end is to facilitate the inner terrain that drives lasting metabolic wellness.
What Patients Should Ask Before Choosing the Best Stem Cell Clinic
Safety, Cell Quality, and Medical Oversight Matter
Patients should ask clear questions before treatment:
What is the stem cell source?
Are the cells UC-MSCs from umbilical cord tissue?
Is donor screening performed?
Are sterility, viability, and endotoxin testing available?
Is the treatment supervised by a physician?
Is there a medical review before treatment?
Are blood tests reviewed before therapy?
Is follow-up monitoring included?
Are expectations explained honestly?
The best stem cell clinic should be transparent. It should explain what stem cell therapy may support, what remains uncertain, and what standard diabetes care must continue.
Stem Cell Therapy Should Work Alongside Standard Diabetes Care
Regenerative Support Is Not a Replacement for Medical Management
And that diabetes care still involves nutrition, physical activity, weight management, glucose monitoring (medications if required), blood pressure control, lipid-lowering therapy where indicated; kidney protection/protective therapies, planning of eye checks, foot checks, cardiovascular risk reduction
Their use in diabetes treatment should be positioned as an adjunct, investigational, and not standard of care. Patients have to work with their doctor to continue using insulin or other glucose-lowering drugs.
Conclusion: A Responsible View of Stem Cell Therapy for Diabetes
The best stem cell clinic is not the one that promises the most. It is the one that provides an honest account of diabetes.
You will note that stem cell therapy for diabetes may be mentioned as an adjunct in select patients, particularly if the targeted outcomes include inflammation, insulin resistance, and/or oxidative stress pathways (angiogenic mediators per local micro-environment), vascular health, and metabolic tissue signaling. It should, however, never be touted as a silver bullet or an alternative to legitimate diabetes care.
Meaning, if you are one of those patients with insulin resistance (which these days is just about everybody), the actual goal was never a lower number on your blood sugar. To augment the metabolic milieu, preserve organ function in the long term, and tailor a safe, feasible personalized treatment paradigm.
FAQ: Stem Cell Therapy for Diabetes and Insulin Resistance
Can stem cell therapy cure diabetes?
No. Stem cell therapy should not be presented as a cure for diabetes. Current research is still developing, and results can vary between patients. It should be discussed as a supportive and investigational approach.
Can stem cell therapy help insulin resistance?
UC-MSCs are being studied for their possible role in inflammation balance, oxidative stress regulation, and metabolic tissue signaling, which may be related to insulin resistance. However, more clinical evidence is needed, and patients should maintain standard diabetes care.
Will I be able to stop insulin after stem cell therapy?
No responsible clinic should promise insulin discontinuation. Any medication changes should only be made by the patient’s treating physician based on glucose monitoring, lab results, and safety.
What tests should be checked before stem cell therapy for diabetes?
Important tests may include HbA1c, fasting glucose, fasting insulin, C-peptide, kidney function, liver function, lipid profile, urine albumin, inflammation markers, blood pressure, and complication screening.
How do I choose the best stem cell clinic for diabetes?
Look for transparent medical evaluation, proper cell sourcing, donor screening, sterility testing, viability testing, physician supervision, realistic communication, and follow-up care. Avoid clinics that promise a cure or guaranteed medication withdrawal.