

Although transfusion of mesenchymal stem cells (MSCs) have remarkable effects in acute liver failure and chronic hepatitis, they show poor engraftment ability when used for treatment.
A hepatic disorder is not one disease. Includes fatty liver, viral hepatitis, alcohol injury of the liver, autoimmune disease from in⁄ with any degree (level) of livery fibrosis or cirrhosis and chronic inflammatory hepatic stress In many patients, the concern starts with high liver enzymes numbers or fatigue (or other causes), and fat in a fatty-liver ultrasound study, borderline/high C-reactive protein levels as well, increased inflammation markersearly fibrosis. Others may have a chronic condition where their liver is already not functioning properly (decreased albumin, increased bilirubin or other clotting abnormalities) and they are beginning to develop ascites.
Hence, patients often look for stem cell options including both: (1) Stem Cell Therapy and (2) DFPP as a more general liver support program. Hence, they are not only asking the way to reduce one lab value. They seek to determine if the liver environment may be sustained more effectively by identifying balance of inflammation, fibrosis signaling and circulation and communication for tissue repair.
Honesty must be the start of a responsible conversation. The designation of stem cell therapy for hepatic disorder is the inadvisable choice, not a genuine cure It should not substitute hepatologist-led care, antiviral therapy for hepatitis B or C, abstinence from alcohol use disorder, weight management in obesity and steatosis patients with nonalcoholic fatty liver disease (NAFLD), metabolic intervention to you had ascites regularly medication assessment cancer screening transplant evaluation when appropriate organ transplantation) be carried out as support people who need emergency treatment.
A Case for the Microenvironment in Liver Disease
The liver is an extremely dynamic organ. The liver processes nutrients and filters blood, regulates metabolism while the liver produces proteins that support immune surveillance to keep us clear of toxins. In fact, repeated liver injury can lead to the local microenvironment becoming fibrogenic and skewed toward inflammation, oxidative stress, immune activation and vascular dysfunction.
The turning point is fibrosis. This occurs when the damaged area does not heal, and scar-like tissue forms. Early fibrosis may still be biologically pliable. Late, however advanced cirrhosis reflects deeper structural change and greater clinical risk.
This is why talks about stem cell therapy need to be delineated into phase of the disease and not a one-stop panacea for all liver diseases.
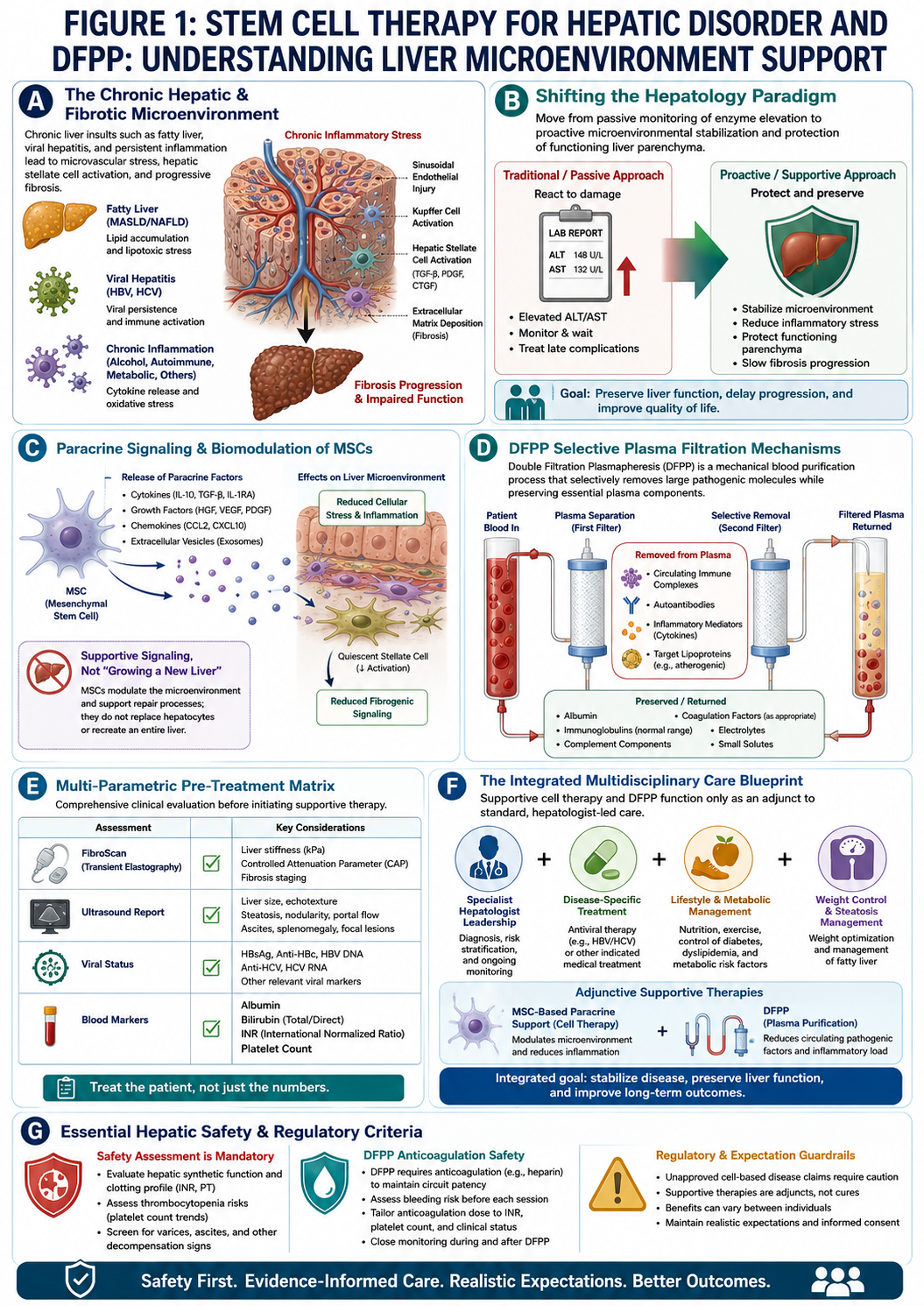
Figure 1: Stem Cell Therapy for Hepatic Disorder and DFPP: Liver Microenvironment Support, MSC Signaling, and Selective Plasma Filtration
Hepatic Disorders: How Stem Cell Therapy May be Discussed
Mesenchymal stem cells, or MSCs are the most widely studied type of cell in this area of liver disease research. MSC stem cells are studied because in-depth research protocols were designed based on the using of their potential biological signals for influencing inflammation, balance between immune effectors and triggers for oxidative stress pathways which could be involved into modulation applying auto-, angiogenesis or fibrosis-associated pathway.
One such concept is paracrine signaling. This implies that stem cells are able to release cytokines, growth factors, extracellular vesicles and other communicating molecules toward nearby cells.
The purpose should not be “to grow a new liver” for hepatic disorder. A better explanation is that stem cell therapy might enhance the liver microenvironment, mitigate inflammatory stress and regulate repair signaling under certain settings. Recent reviews on stem cells for chronic and end-stage liver disease point out it is a promising yet active field of research, which seems to face challenges in standardization generation (engineering), target population identification and clinical translatability.
Potential Place for DFPP in Liver Support
Double filtration plasmapheresis (DFPP) is a blood purification technique that works by separating plasma and filtering selectively large molecules. It is not a liver cure. DFPP may be used for the removal of specific circulating burdens like immune complexes, inflammatory mediators, lipoproteins or large plasma proteins as determined by physician preference and patient condition in supportive care conversations.
This is what conceptually separates DFPP from stem cell therapy. DFPP is based on selective plasma filtration. Research on Biological Signaling and Immune Modulation by Stem Cell-Based Care DFPP may be offered by a clinic as hope to reduce systemic inflammatory or metabolic burden pre- and/or post-regenerative support in selected patients, IF done on an individualized basis.
DFPP is a technique that expels disease-related substances including autoantibodies, immune complexes and lipoproteins from plasma with higher selectivity than conventional plasma exchange – as highlighted by recent reviews.
What a Responsible Clinic Should Review First
Before discussing stem cell therapy or DFPP, a clinic should review the exact hepatic disorder, liver enzyme trends, bilirubin, albumin, INR, platelet count, fibrosis score, ultrasound or FibroScan findings, viral hepatitis status, alcohol history, fatty liver risk, autoimmune markers, cholesterol profile, kidney function, medications, cancer history, and hepatologist recommendations. A patient with fatty liver is very different from a patient with decompensated cirrhosis. Patient selection is essential.
Safety and Realistic Expectations
Safety is important because liver patients can have clotting problems, low platelets, increased risk of infection and fluid overload as well stress on the kidney metabolism, or anemia or medication complexity. Patients may inquire about these factors: cell source, donor screening (for transfusion-transmissible pathogens), sterility testing, viability and potential shelf-life of the product weight by endotoxin what goals guided DFPP filtration approach to how much anticoagulation is safe aggression route clinical relevance safety monitoring done in follow-up.
Any clinic must not claim that stem cell therapy or DFPP can cure hepatic disorder, reverse cirrhosis, be an alternative to transplant, stop all medication and normalize every liver marker. Warnings from FDA also caution patients about cell-based products that are marketed for wider disease claims utilize unapproved other than as therapy.
Conclusion
Hence the interests are on stem cell research, therapy for stimulation of these cells to work optimizedly such that their therapeutic potential against hepatic disorders were better supported while duplicating or replenishing blood purification supports them in a subgroup usually called DFPP. This made liver disease feel slow, complicated, and uncertain.
The best way to conceptualize this area is not as a cure but rather an incremental medical model; when possible, alleviating the well-being-draining proficient burden of cirrhosis by offsetting supportive administration through other alive balances occurring amongst inflammation and fibrosis signaling while allowing restoration in quality-of-life facets.secondary care should continue with salience toward managing burdens associated PSG source factors/pathways across progressive lifestyle modifications.