

Stem Cell Therapy for Autism: A Science-Based Look at Whole-Child Support
Autism is not one single pattern. It is a neurodevelopmental condition that may affect communication, social connection, sensory processing, sleep, attention, learning, emotional regulation, and daily routines. Some children need help with language. Some struggle with sensory overload. Others may have sleep issues, digestive sensitivity, repetitive behaviors, or difficulty adapting to change.
This is why many families search for stem cell options and stem cell therapy for Autism. Most parents are not looking for a shortcut. They are looking for another layer of support when progress feels slow, uneven, or difficult to predict.
A responsible discussion must begin with honesty. Stem cell therapy should not be described as a cure for Autism. It should not replace speech therapy, occupational therapy, behavioral support, pediatric care, educational planning, or family-based intervention. Autism is not something to “erase.” The better question is whether stem cell research may help us understand immune balance, inflammation, cell signaling, and supportive biological care in selected children.
A Different Way to Understand Autism Biology
Autism is usually discussed through behavior and development, but biology may also matter. Some research has explored links between Autism and immune dysregulation, inflammatory signaling, oxidative stress, gut-brain communication, and altered cellular signaling.
This does not mean every child with Autism has inflammation. It also does not mean inflammation “causes” Autism by itself. Autism is complex and highly individual. But these biological layers help explain why researchers are studying stem cell therapy as a possible supportive approach, not a cure.
Why Stem Cells Are Being Studied
The most common stem cell discussion in Autism research involves mesenchymal stem cells, or MSCs. MSCs are studied because they may release biological signals that interact with immune cells, inflammatory pathways, and tissue communication systems.
The key concept is paracrine signaling. This means stem cells may release cytokines, growth factors, extracellular vesicles, and other molecules that communicate with surrounding cells.
For Autism, the goal should not be explained as “new brain cells” or “instant brain repair.” A more accurate explanation is that stem cell therapy is being studied for immune modulation, inflammation balance, and cellular communication support.
What Current Research Suggests
The potential use of umbilical cord stem cells and MSCs derived from the human Wharton’s jelly have been investigated in small clinical trials settings for children with Autism. A few studies reported that in selected children treatment was well tolerated, and some families or investigators observed improvement without having quantitative measures.
Yet, the evidence continues to be gathering. Most studies are small, early-phase or hindered by variations in cell source, dose administered and route of administration as well as follow-up duration and outcome measurement.
The honest truth: stem cell therapy for Autism has exceptionally well-vetted study leading us to believe that this may be the future standard of what becomes a treatment. Better controlled trials and longer follow-up are required.
What Families May Hope to See
Families often wonder what better will be like. Clients can report better sleep, smoother transitions (check if this is family reported as well), improved focus, more eye contact and social engagement or communication in general with the child, reduced sensory sensitivity or even just a higher level of ease being touched next to increased verbal attempts & participation at home/meaningful environments especially through assessing therapists that involve play.
These modifications can be important, though they should never promised. This change reflects the development of autism over time, and improvement can also result from speech therapy or other treatments such as occupational therapy, behavioral support, sleep hygiene education, improved nutrition in childhood / adolescence into early adulthood (like a healthy diet), positive home environment.
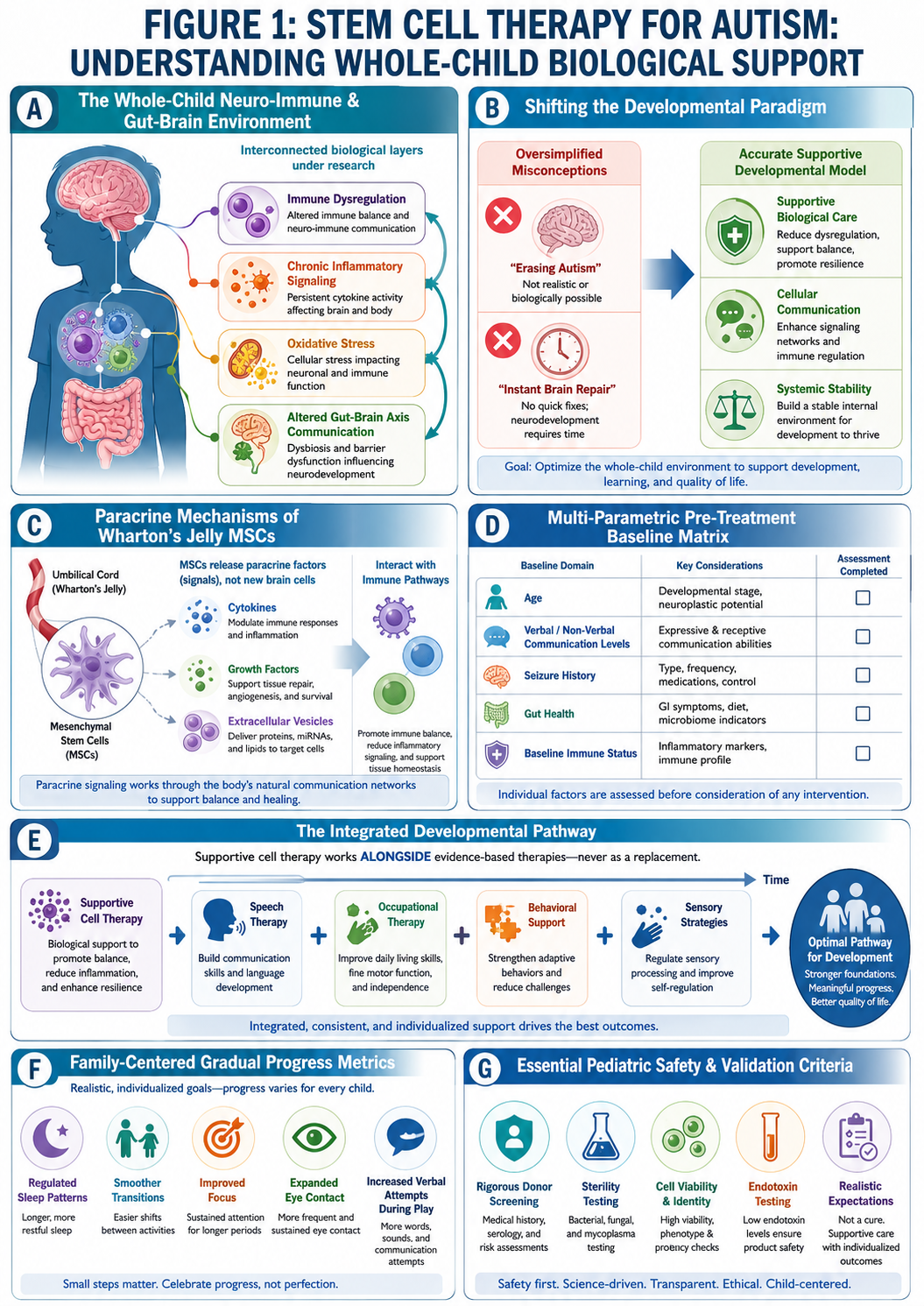
FIGURE 1: STEM CELL THERAPY FOR AUTISM: UNDERSTANDING WHOLE-CHILD BIOLOGICAL SUPPORT
Figure 1 Key:
(A) The Whole-Child Neuro-Immune & Gut-Brain Environment: Visualizing the interconnected biological layers under research, including immune dysregulation, chronic inflammatory signaling, oxidative stress, and altered gut-brain axis communication.
(B) Shifting the Developmental Paradigm: Transitioning the clinical objective from oversimplified misconceptions of “erasing autism” or “instant brain repair” toward supportive biological care, cellular communication, and systemic stability.
(C) Paracrine Mechanisms of Wharton’s Jelly MSCs: Illustrating how umbilical cord-derived mesenchymal stem cells release bioactive signaling molecules (cytokines, growth factors, and extracellular vesicles) to interact with immune pathways, rather than creating “new brain cells.”
(D) Multi-Parametric Pre-Treatment Baseline Matrix: Highlighting the critical individual factors required before consideration, including age, verbal/non-verbal communication levels, seizure history, gut health, and baseline immune status.
(E) The Integrated Developmental Pathway: A multi-layered timeline demonstrating that supportive cell therapy operates strictly alongside—and never replaces—core developmental interventions (speech therapy, occupational therapy, behavioral support, and sensory strategies).
(F) Family-Centered Gradual Progress Metrics: Mapping out realistic, non-guaranteed outcomes reported by families, such as regulated sleep patterns, smoother transitions, improved focus, expanded eye contact, and increased verbal attempts during play.
(G) Essential Pediatric Safety & Validation Criteria: Mandatory laboratory and clinical guardrails emphasizing rigorous donor screening, sterility, cell viability, endotoxin testing, and the firm calibration of realistic, non-curative expectations.
Any responsible clinic is likely to explain that results depend on age, symptom profile, communication level (verbal/non-verbal), seizure history (idiopathic or symptomatic epilepsy), sleep quality, gut health and immune status as well current therapies and follow up support.
Safety Comes Before Hope
Safety is essential. Families should be cautious of any clinic that claims stem cell therapy for Autism is guaranteed, risk-free, permanent, or curative.
A proper medical review should include diagnosis, developmental history, seizure history, allergies, medications, infection history, immune conditions, sleep problems, behavior concerns, and overall medical stability.
Families should ask about cell source, donor screening, sterility testing, viability, endotoxin testing, cell identity, route of administration, physician supervision, and follow-up monitoring.
Stem Cell Therapy Should Work Alongside Developmental Care
The best framework is not “stem cell instead of therapy.” It is supportive biological research alongside established developmental care.
Speech therapy, occupational therapy, behavioral support, sensory strategies, sleep routines, school planning, and family coaching remain central. If stem cell therapy is considered, progress should be tracked gradually and realistically.
Conclusion
The interest in stem cell research and stem cell therapy for Autism is understandable. Families want more options and clearer paths forward.
Stem cell research is scientifically interesting because of immune modulation, inflammation balance, paracrine signaling, and whole-child biological support. However, it should not be described as a cure or replacement for developmental therapy.
The strongest approach is careful medical review, safety screening, continued autism support, honest explanation, and realistic expectations.