

Rheumatoid arthritis (RA) is a significant modern rheumatology challenge, an incipient chronic [state of systemic inflammation targeting the synovial joints. This is not just arthritis or joint pain; it is a degenerative autoimmune disease in which the immune surveillance mechanisms incorrectly mark healthy synovial tissues as targets. Severity is high and can cause destruction of cartilage, bone erosion as well as affecting other organs such vessels like in case of cardiovascular involvement. As far as impact is concerned, this is devastating for the patient, leading often to motor disabilities and lack of functional independence.
Pharmaceutical interventions have come a long way, however many patients are either non-responsive or experience severe adverse side effects. This the urged need for exploring out of regenerative medicine. Stem cell Therapy Thailand: a new paradigm enabled by UC-MSCs. These advanced biological therapies aim to go beyond symptom management to reset the immune environment, offering hope for a cure where standard medicines have not been able to provide satisfactory relief.
1.Pathophysiological Mechanisms and Clinical Manifestations
We will review the pathogenesis of Rheumatoid Arthritis which results from an interaction between genetic predisposition and environmental triggers that ultimately leads to loss of self-tolerance. At the molecular level, the disease is characterized by infiltration of activated T cells, B cells and macrophages into the synovium. These cells release a potent mix of pro-inflammatory cytokines, including Tumor Necrosis Factor-alpha (TNF-α), Interleukin-6 (IL-6) and Interleukin-1 (IL-1β). Such events trigger a cytokine storm which in-turn, activates synovial fibroblasts to take on an aggressive tumor-like phenotype, termed the pannus.
Through the growth of the pannus, matrix metalloproteinases (MMPs) are secreted and they begin to degrade cartilage matrix. At the same time, this inflammatory milieu promotes osteoclastogenesis with local bone loss. Clinically, this presents as symmetrical joint swelling, morning stiffness and very frequently fatigue. Without it structural integrity crumbles and various deformities arise such as ulnar drift, limiting manual dexterity. Because inflammation is systemic, patients frequently develop associated conditions including vasculitis, with the consequent need for targeted management.
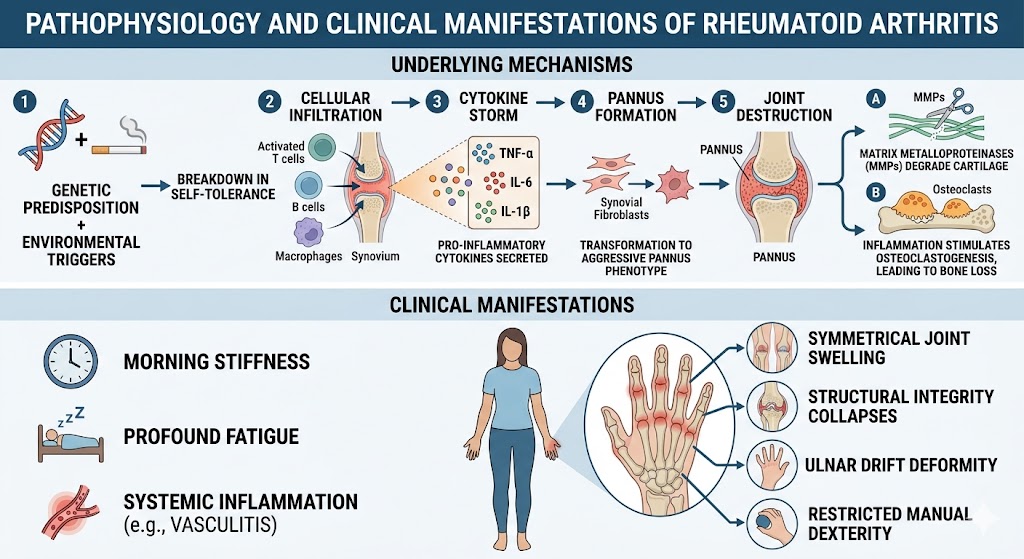
Figure 1: Pathophysiological Mechanisms and Clinical Manifestations
2.Conventional Treatment Modalities and Limitations
At present, the way it is clinically done uses a stepwise strategy beginning with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), and then proceeds to include Disease-Modifying Antirheumatic Medicines (DMARDs) including methotrexate. In refractory cases, cytokine-specific biological agents are employed. Although these treatment has advance the results, however, they’re nowhere in proximity to best.
One of the main limitations of conventional DMARDs is that they have to be taken for life, which causes systemic immunosuppression and can lead to infections. Additionally, 30%–40% of patients are categorized as inadequate responders in achieving low disease activity. These are also anti-inflammatory, but they do nothing to restore structural harm caused in already-damaged cartilage and bone, so patients still experience chronic mechanical pain. It results in a cycle of dependence on drugs that may grow ineffective or develop organ toxicity over time.
3.Therapeutic Potential and immunomodulatory roles of UC-MSCs
UC-MSCs, Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue engineering, 2001. 7(2): p. 211–28. Following the collection of an umbilical cord (which will otherwise be discardedat birth), UC-MSCs have a few key advantages over any adult-derived bone marrow-derived cells as far as they are concerned:They proliferate more readily in culture; and They have powerful immunomodulatory properties to suppress T-cell proliferation and differentiation into effector T-cells via secretion of mediators such as IL-6, IFN-gamma. These cells have a distinct capability to detect local inflammation temperature. In high-inflammation setting, UC-MSCs take effects through direct cell-cell contact and bioactive paracrine factors.
The first main mechanism is the promotion of Tregs, which helps maintain peripheral tolerance and prevent inflammatory Th1 or Th17 immune overactivity. UC-MSCs also produce inhibitory factors of dendritic cell maturation such as Indoleamine 2,3-dioxygenase (IDO) and Prostaglandin E2 (PGE2). Meanwhile, these cells help in tissue repair by secreting growth factors, such as TGF-β, which induces native chondrocytes to synthesize new collagen. The simultaneous effect of ceasing to convert mass destruction of autoimmunity, along with the transaction green signal conditioning a different pro-regenerative accessible surrounding city, is why stem cell Therapy Thailand has become a focus location for those researching cure that works holistically. These cells essentially serve as biological pharmacists with the ability to silence inflammation at a specific site through signals.
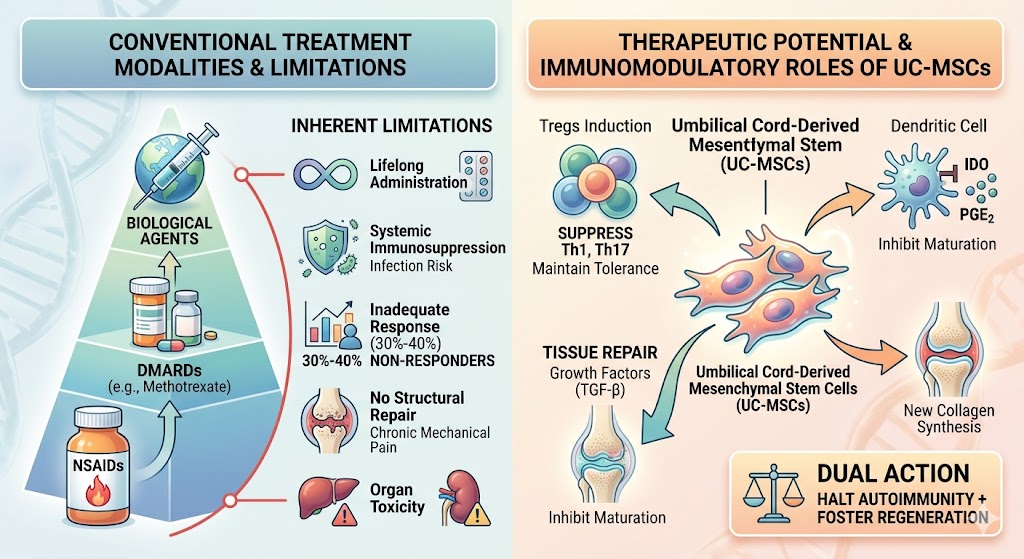
Figure 2: Conventional Limitations and Therapeutic Potential and Immunomodulatory Roles of UC-MSCs
4. Future Trajectory of MSC Research within Thailand
Thailand has rapidly positioned itself as a global hub for regenerative medicine, specifically in the clinical application of mesenchymal lineages. The future of UC-MSCs in this region is supported by a robust infrastructure of specialized clinics and a regulatory environment encouraging biotechnological innovation. The reason why stem cell Therapy Thailand is gaining such momentum is the combination of world-class medical expertise and the increasing accessibility of advanced cell-based products.
Looking ahead, the integration of UC-MSCs into standard rheumatological care in Thailand is expected to move toward personalized protocols. Researchers are currently investigating the use of primed MSCs to enhance their homing capabilities to inflamed joints. Thailand’s strategic focus on medical tourism ensures the nation remains at the forefront of this field, providing a viable destination for patients seeking alternatives to lifetime pharmaceutical dependence. The focus is shifting from simple injection to a comprehensive therapeutic experience combining cellular biology with precision monitoring. As more clinical data emerges from local institutions, confidence in these therapies continues to rise, attracting international interest into the Thai biotech sector.
In summary, the autoimmune landscape is shifting significantly. While traditional therapies provide a foundation, drug toxicity and incomplete efficacy remain problematic. The utilization of UC-MSCs offers a sophisticated biological solution addressing root causes of synovial inflammation rather than just symptoms. By leveraging the natural reparative qualities of umbilical cord cells, clinicians provide a path toward joint restoration.
As evidence supporting stem cell Therapy Thailand grows, these cellular interventions represent the next frontier. For those living with Rheumatoid Arthritis, transitioning from chronic management to regenerative healing offers renewed possibility. Ongoing advancements in Thailand ensure access to high-tier biological tools, marking a pivotal moment against degenerative conditions. This evolution promises a future where long-term remission and physical restoration become primary goals, reducing the global disability burden. The synergy between cell biology and Thai clinical expertise sets a new benchmark for treating autoimmune pathologies.