

- Introduction to Metabolic Dysfunction
Diabetes condition is a common metabolic disorder defined by abnormal glucose homeostasis induced by insulin resistance, defective secretion of insulin, or both. Long-term insulinopenic hyperglycemia affects the kidneys, nerves, and eyes as well as leading to cardiovascular damage. The impact of diabetes extends beyond blood sugar levels, it is a systemic disease characterized by inflammation, oxidative stress and metabolic imbalance.
Patients have fatigue, unstable energy levels, delayed wound healing and long-term complications like neuropathy, nephropathy, vascular issues, etc. Although standard care aims at glucose control with lifestyle modification, oral agents, and insulin therapy. Those are still the cornerstones of management.
But increasing evidence has implicated oxidative stress, mitochondrial dysfunction, and inflammation in the development of diabetes. This has been followed by growing interest in adjunctive strategies such as umbilical cord-derived mesenchymal stem cells (UC-MSCs) and metabolic support compounds alpha-lipoic acid (ALA).
- Pathophysiology of Diabetes Progression
The progression of diabetes involves a complex interplay between insulin resistance, pancreatic β-cell dysfunction, chronic inflammation and oxidative stress. In type 2 diabetes, the cells become less responsive to insulin, which forces the pancreas to compensate. With time, beta cells may become dysfunctional, leading to persistent hyperglycemia.
Simultaneously, oxidative stress is a key player. High glucose levels lead to excessive generation of reactive oxygen species (ROS) that damage the structure, abrogate insulin signalling and foster complications like neuropathy and endothelial dysfunction. This undercurrent inflames the process further, creating chronic low-grade inflammation.
But diabetes is more than just a disorder of glucose metabolism, with these mechanisms revealing it also as one possessing immune imbalance, cellular stress and gradual tissue damage. This realization bolsters interest in therapies that target the biological ecology, rather than just blood sugar levels.
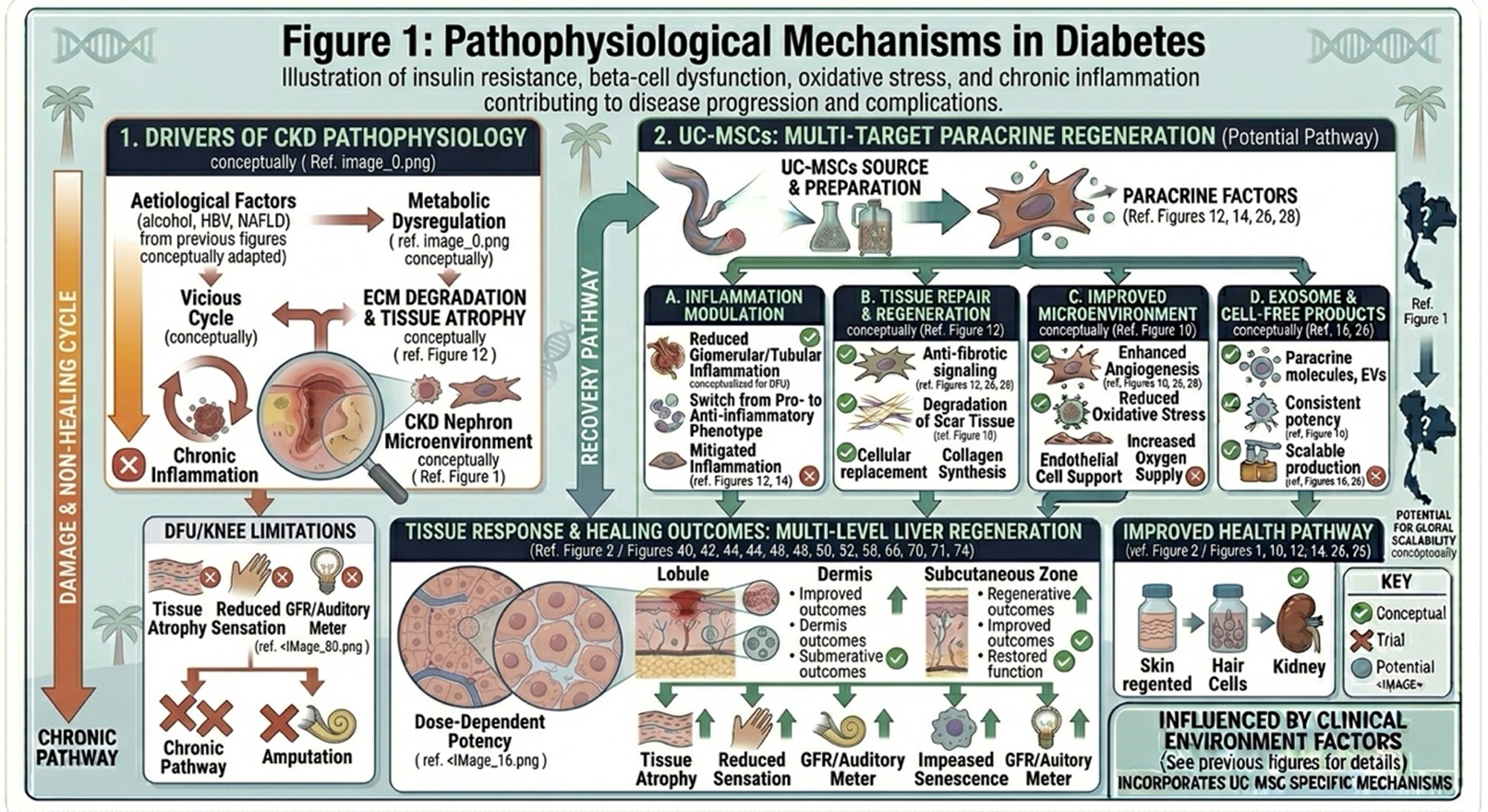
Illustration of insulin resistance, beta-cell dysfunction, oxidative stress, and chronic inflammation contributing to disease progression and complications.
- Limitations of Conventional Treatment Alone
Standard treatments for diabetes are very effective at controlling blood glucose levels and reducing complications. Drugs like metformin, insuline and newer agents (SGLT2 inhibitors, GLP-1 receptor agonists) have led to better patient outcomes. But these therapies only target metabolic control rather than cellular repair. They do not directly cure oxidative damage, restore beta-cell function, or resolve chronic inflammation. This potentially explains why glycemic control is only partially effective, as a number of patients continue to experience disease progression despite good glycemic control. Also, neuropathy and vascular dysfunction are long-term complications that may remain over time even if glucose levels are maintained. This has resulted in growing interest surrounding supportive approaches potentially conducive to cell protection, improvement of oxidative stress and metabolic resilience.
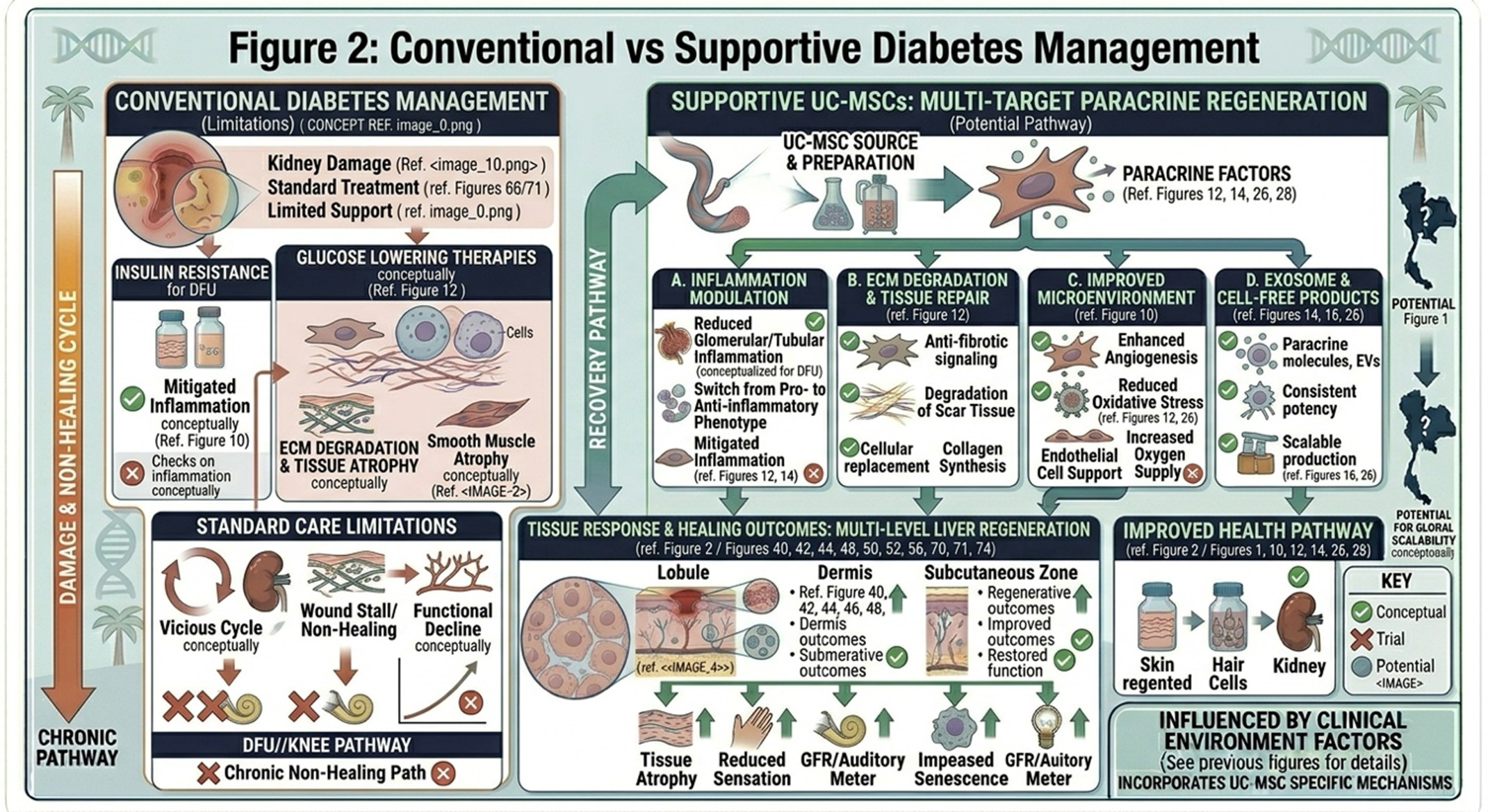
Comparison between standard glucose-lowering therapies and adjunctive strategies targeting inflammation, oxidative stress, and cellular function.
- Potential Benefits of UC-MSCs in Diabetes Support
UC-MSCs are being investigated for their paracrine effects involving the metabolic and inflammatory milieu. These cells secrete bioactive molecules (including cytokines, growth factors and extracellular vesicles), which could participate in regulating immune response and supporting tissue repair.
Potential Effects of UC-MSCs in Diabetes Research
- Modulation of inflammation
- Support of pancreatic beta-cell function
- Improvement in insulin sensitivity
- Reduction in oxidative stress
Results from some preclinical and early clinical studies show that MSC-based approaches may be associated with improved glycemic control, as well as metabolic parameters when compared with baseline in select patients. However, results are mixed and further large-scale clinical trials are required to confirm longer term efficacy and safety.
UC-MSCs may be a potential investigational adjunct to standard diabetes care under appropriate medical supervision, but should not serve as a stand-alone replacement for standard diabetes management.
- Role of Alpha-Lipoic Acid (ALA) in Metabolic and Nerve Support
Alpha-Lipoic Acid (ALA) is a naturally occurring redox active thiol that participates in mitochondrial energy metabolism. Some people have studied it in the context of diabetes (due to its potential to reduce oxidative stress and support nerve function).
ALA is known to:
- Neutralize reactive oxygen species (ROS)
- Improve mitochondrial function
- Support insulin sensitivity
- May help relieve symptoms of diabetic neuropathy
Clinical studies suggest that ALA supplementation can improve neuropathy symptoms like pain, burning sensation and numbness in some individuals. It might also help improve glucose utilization in some circumstances.
However, ALA is one of the more established supportive compounds available for use in diabetes care, and like all supportive techniques generally offers modest effects rather than cure. Outcomes are determined by dosage, formulation and patient selection.
- The Role of Specialized Medical Centers
As demand for integrative metabolic care increases, dedicated clinics are incorporating medical management with regenerative approaches and targeted nutritional support. Some centers may provide structured programs encompassing metabolic assessment, monitoring, and personalized treatment planning.
Countries like Thailand have experienced the availability of advanced medical technologies and well-trained clinicians which has promoted integrative approaches to diabetes management. But, the value of such programs is not just in therapies offered but also with proper patient screening, safety protocols and setting realistic expectations.
Perhaps a consortium of benign (non-HT) therapies aimed at inhibiting progression could be integrated into an ideal model, ultimately together combining conventional care and carefully selected supportive treatment to provide better management.
- Final Thoughts on Supportive Diabetes Care
Diabetes is a chronic, multifactorial condition that needs continuous care. And, though conventional therapies are vital to the treatment of Alzheimer’s disease, increasing scientific insight into the roles played by inflammation, oxidative stress and cellular dysfunction has paved the way for potential supplementary strategies.
UC-MSCs are emerging as a potential means for modulating inflammation and supporting metabolic function, whereas ALA has an established role in protecting against oxidation that may translate into benefits to nerve health and cellular metabolism.
The most responsible way to look at these therapies is as adjunctive, not curative. Results may vary and all medical treatment should be discussed with a physician.
The future of diabetes management could be more integrative than ever for metabolic control, cellular support, and personalized medicine to improve clinical outcomes and quality of life (QoL) as research still ongoing.