

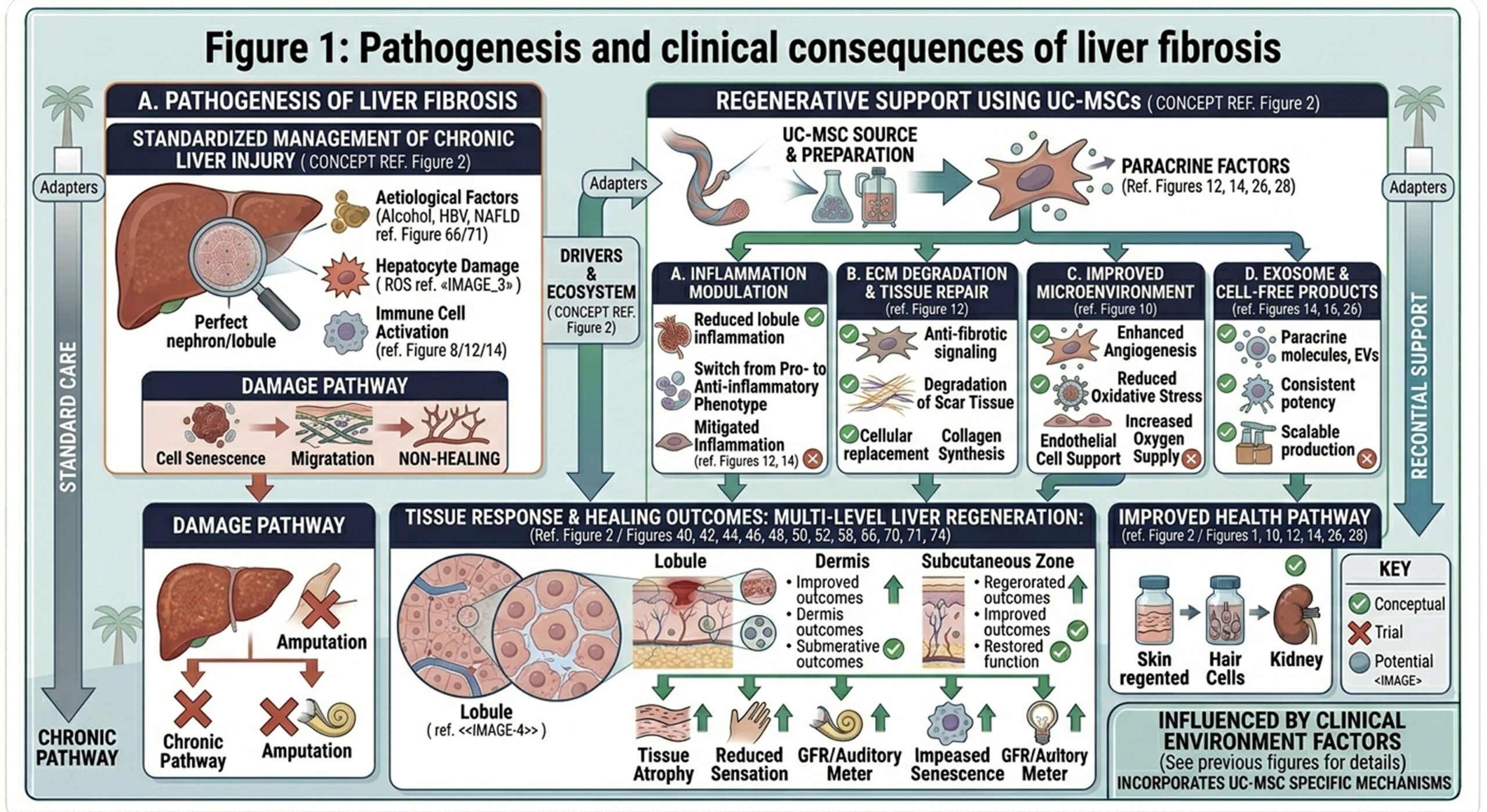
Chronic liver injury is a serious public health issue worldwide and can progress to cirrhosis, one of the most severe forms of chronic liver disease. Regardless of whether the underlying injury is viral hepatitis, alcohol-related or nonalcoholic fatty liver disease, chronic tissue injury may induce recurrent cycles of inflammation and fibrosis. Normal liver tissue is gradually replaced by fibrotic bands and nodular distortion, which decreases the ability of the organ to perform its critical functions. As liver function deteriorates, patients can develop jaundice, fluid retention, portal hypertension, encephalopathy and other life-threatening complications. Conventional medical care can control symptoms and slow some mechanisms of progression, but rarely reverses established fibrosis. This has brought regenerative strategies into focus, and UC-MSCs are being investigated as a potential biological method to promote liver repair beyond the limits of standard therapy.
- Pathogenesis and clinical burden of liver fibrosis
Cirrhosis development is mediated by a complex cascade of maladaptive cellular injury and repair. In which hepatic stellate cells are one of the main players. In a healthy liver, these cells are relatively quiescent, but under chronic inflammatory stress they convert into fibrogenic myofibroblasts and start to produce high levels of extracellular matrix components notably collagen. This abnormal buildup of the matrix progressively disrupts normal liver architecture and impedes blood flow, nutrient exchange, and tissue function.
Early on, fibrosis may progress without symptoms. However, at a certain point of damage, there are systemic consequences. Protein synthesis falls off, albumin levels drop, detoxification fails and toxins such as ammonia can accumulate in the circulation wreaking havoc on brain function and general health. At this point, cirrhosis is not merely a structural abnormality of the liver; it is a multisystem disorder that interferes with daily living, physical stability and survival. So treatment strategies that focus on merely slowing decline are frequently not sufficient, and regenerative approaches have attracted so much interest.
- Traditional treatment strategies and their limitations
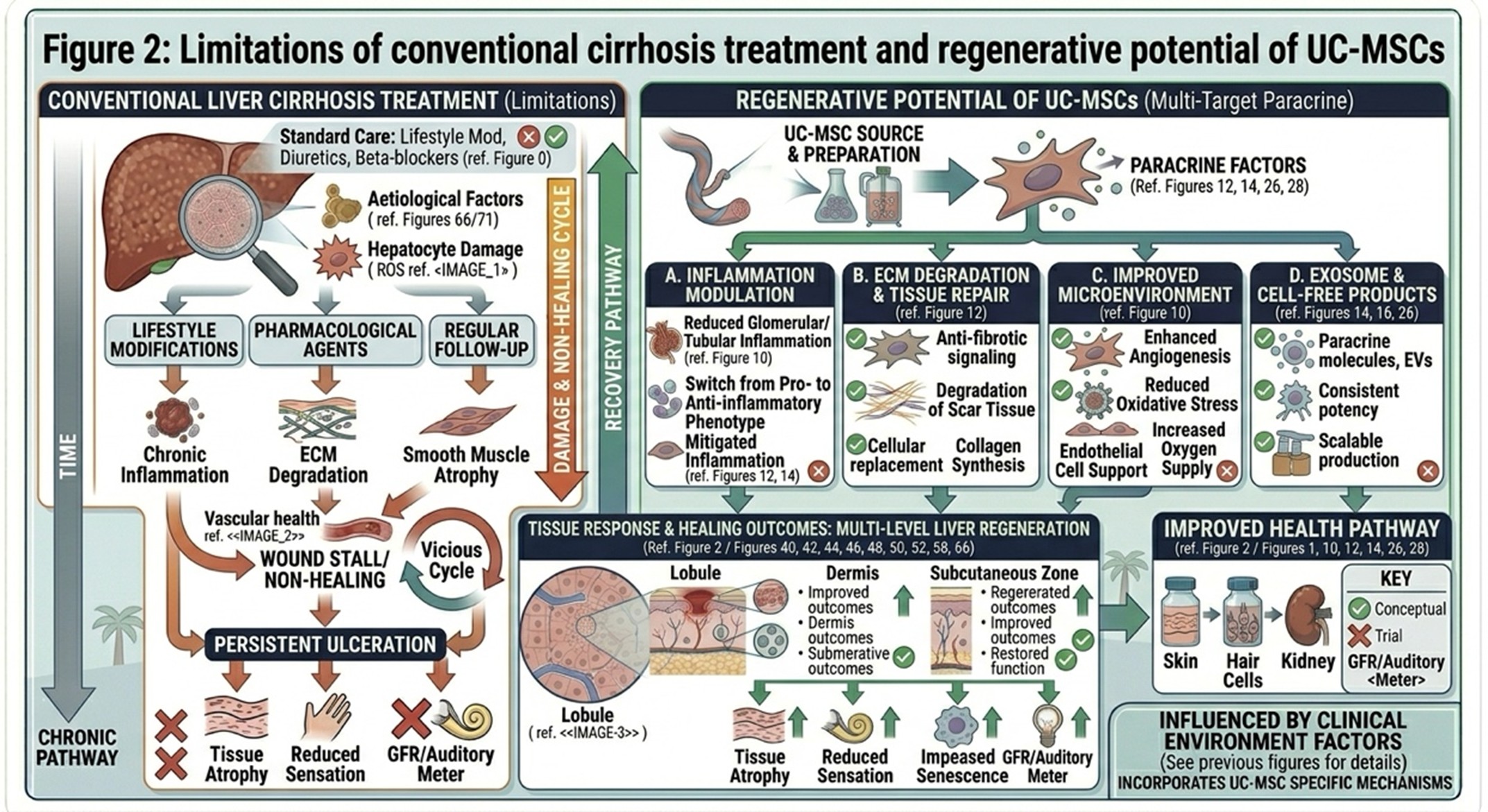
Conventional cirrhosis management primarily involves controlling the underlying trigger along with minimizing complications. Antiviral therapy is given to patients with viral hepatitis and dietary recommendations in terms of weight control, glycemic management, and lifestyle modification. These actions are critical because they can prevent additional injury. But once scar tissue becomes dense, standard treatment can’t do much to eliminate it or restore altered liver architecture.
Symptomatic-based medications, like diuretics to relieve fluid overload or beta-blockers for portal hypertension, can enhance short-term stability but do not regenerate liver tissue. Liver transplantation is the definitive treatment for patients with end-stage disease. However, transplantation itself is fraught with challenges: donors are limited in number and high risk for surgical complications; the procedure is expensive; and lifelong immunosuppressive therapy is necessary. Those medications can raise the risk of infection and kidney problems and other complications. Such barriers have renewed focus on less invasive, biologically active alternatives that can bridge the divide between symptomatic management and organ replacement.
- Why UC-MSCs are attractive in liver regeneration
The increasing interest in UC-MSCs embodies a broader movement within medicine from treatment that provides supportive care but not biological restoration, to biologically restorative treatments. Umbilical cord-derived mesenchymal stromal cells are generally preferred because they can be obtained non-invasively and expand readily, besides being robustly immunomodulatory. They are also viewed as being attractive for use in allogeneic research settings compared with some other stem cell sources.
UC-MSCs are believed to mediate their effects via several inter-connected mechanisms while administering in the conditions of cirrhosis. Key among these is their ability to migrate to sites of inflammation and tissue damage. Upon arriving to the injured liver niche, they can secrete a variety of signaling molecules including cytokines and growth factors as well as extracellular vesicles. These secreted factors may mitigate ongoing inflammatory activity, regulate fibrogenic pathways and promote tissue repair. Their specific potential to inhibit hepatic stellate cell activation, limit excess collagen deposition and promote matrix remodeling has further attracted research interest.
Another potential advantage is their impact on the immune environment. By initiating macrophage responses and reducing chronic-inflammatory cytokines, UC-MSCs could help modulate inflammatory pathways restoring a more repair-swinging profile. Moreover, they could protect the remaining hepatocytes from apoptoeis and preserve the functional liver tissue that has not been lost. The extensive biological actions have led researchers to consider UC-MSCs as a potential regenerative platform in chronic liver disease rather than just as a narrow, single-target therapeutic agent.
- Stem cell therapy as a modern therapeutic alternative
One reason stem cell therapy has generated so much interest is that living cells may react to the tissue microenvironment in a way that traditional drugs cannot. And while chemical therapies typically target a single pathway or receptor in one manner at a time, UC-MSCs can modulate multiple processes simultaneously. In cirrhosis, the global treatment goal is to move the liver from a state of chronic injury and fibrosis expansion towards a more favorable environment for repair and stabilization.
Another reason why UC-MSCs attracted attention is their relatively low immunogenicity. Because they show less of the surface signals which generally provoke strong immune rejection, they may be more applicable for allogeneic use than most other cell-based products. It allows for more practical preparation, characterization and storage of the cell products for clinical use. Thus, their proposed benefits in cirrhosis include anti-fibrotic signaling, immune modulation, hepatocyte survival support and creation of a microenvironment that may be more permissive to endogenous regeneration.
- Future directions and Thailand’s role in regenerative liver care
Thailand is gaining prominence in the field of regenerative medicine due to its mature biotechnology industry, advanced medical infrastructure, and interest in incorporating cellular therapies into mainstream clinical practice. Support for this country’s development in this area has been laboratory capability, experienced clinicians and ongoing investment in translational medicine. This has provided an opportunity for Thailand to establish itself as a hub for advanced regenerative care, including UC-MSCs-based therapies.
Developments in liver fibrosis research should pave the way for further advances and perhaps put Thailand in consideration as a key partner to help optimize treatment regimens, refine dosing strategies and promote access to quality cell-mediated therapy. A near-laboratory to clinical continuum of science is particularly critical in a field like regenerative hepatology, where therapeutic success relies not only on product quality but also patient selection and protocol design. With knowledge expanding, Thailand is well positioned to make a meaningful contribution during the next wave of liver regenerative medicine.
Conclusion
Patients with cirrhosis had few options except to treat complications and await transplantation for many years. UC-MSC-based therapy represents a new conceptualization of chronic liver disease. In contrast to targeting the consequences of fibrosis alone, regenerative approaches address the global cellular processes responsible for continuous damage. UC-MSCs thus represent a potential step forward in the management of liver disease by addressing inflammatory, fibrogenic signaling and tissue support host-pathogen interactions.
While conventional therapies remain the cornerstone of disease management, regenerative cell-based approaches may herald a long-term shift in the paradigm by which chronic liver injury is addressed. The recent evolution in treatment protocols has made the scope of biologically active cellular therapy for supporting liver recovery with time-frame relevance. In this regard, Thailand’s advancement in stem cell therapy may actually be part of a wider paradigm shift in the treatment of cirrhosis patients.