

THE GROWING BURDEN of neurodegenerative disease is one of the great challenges of modern neurological medicine. Among these conditions, Parkinson’s disease is one of the most functionally disabling diseases in older adults. The disease is characterized primarily by gradual, progressive loss of dopaminergic neurons in the substancia nigra pars compacta that effects motor control and increased dependence through functional disability. In addition to tremor, rigidity and slowed movement, Parkinson’s disease is a major emotional, social and financial burden on patients and caregivers. As the disease progresses, many people additionally develop non-motor complications of Parkinson’s disease – mood disturbance, sleep dysfunction and cognitive decline – all of which can lead to increased loss in quality of life.
- Pathobiology of Parkinson’s Disease
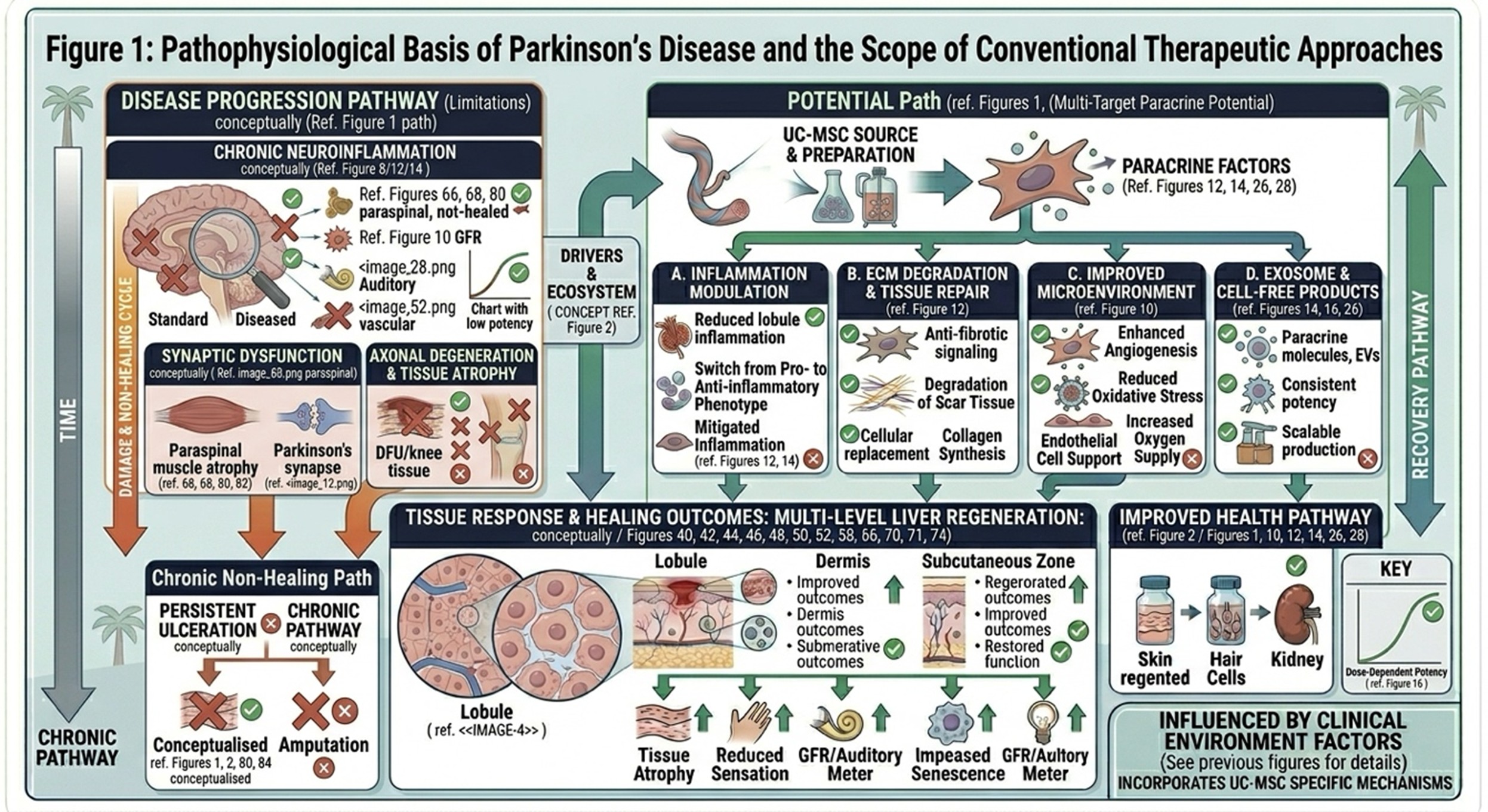
The pathological index of the development of Parkinson’s disease is an abnormal accumulation of misfolded proteins, mainly α-synuclein which aggregate into intracellular inclusions called Lewy bodies. Pathologic protein aggregates disrupt cellular homeostasis, leading to mitochondrial dysfunction, oxidative stress and impaired clearance mechanisms. The resulting opportunities for the processes of damage to potentiate each other lead to a progressively more pro-inflammatory environment in the nervous system, which hastens cell loss among dopaminergic neurons.
The loss of dopamine hampers signaling in the basal ganglia circuit, an essential system for providing coordination to voluntary movement. This dysfunction is at the basis of classic motor manifestations of the disease: bradykinesia, resting tremor, rigidity and postural instability. Significantly, Parkinson’s disease is not limited to motor pathways. With time, pathological alteration can involve wider neural circuits, shedding light in part on the development of cognitive, behavioral and emotional disturbances in late-stage disease.
- Limitations of Established Parkinson’s Therapies
Levodopa, a dopamine precursor that can palliate motor symptoms, particularly in the early and mid-stages of disease, has been enshrined as the standard pharmacologic strategy to treat Parkinson’s disease for many years. Although generally effective initially, these medications can cause motor fluctuations along with levodopa-induced dyskinesias to some extent over time; later they become more difficult to manage. Other medications, such as dopamine agonists and MAO-B inhibitors, may offer some additional symptomatic benefit but do not slow down the underlying neurodegenerative process.
Deep brain stimulation (DBS) is an additional therapeutic option for patients where medication response has become inconsistent. But DBS is invasive, not suitable for all patients, and remains mostly a symptom-control approach to disease rather than a ratifier of the underlying process. As a whole, current standard therapies are still important, but they are compensatory not restorative. This continuing gap has led to interest in regenerative and cell-based approaches that have the potential to provide more broad biological support.
- The Emergence of Cell-Based Neurorestorative Strategies
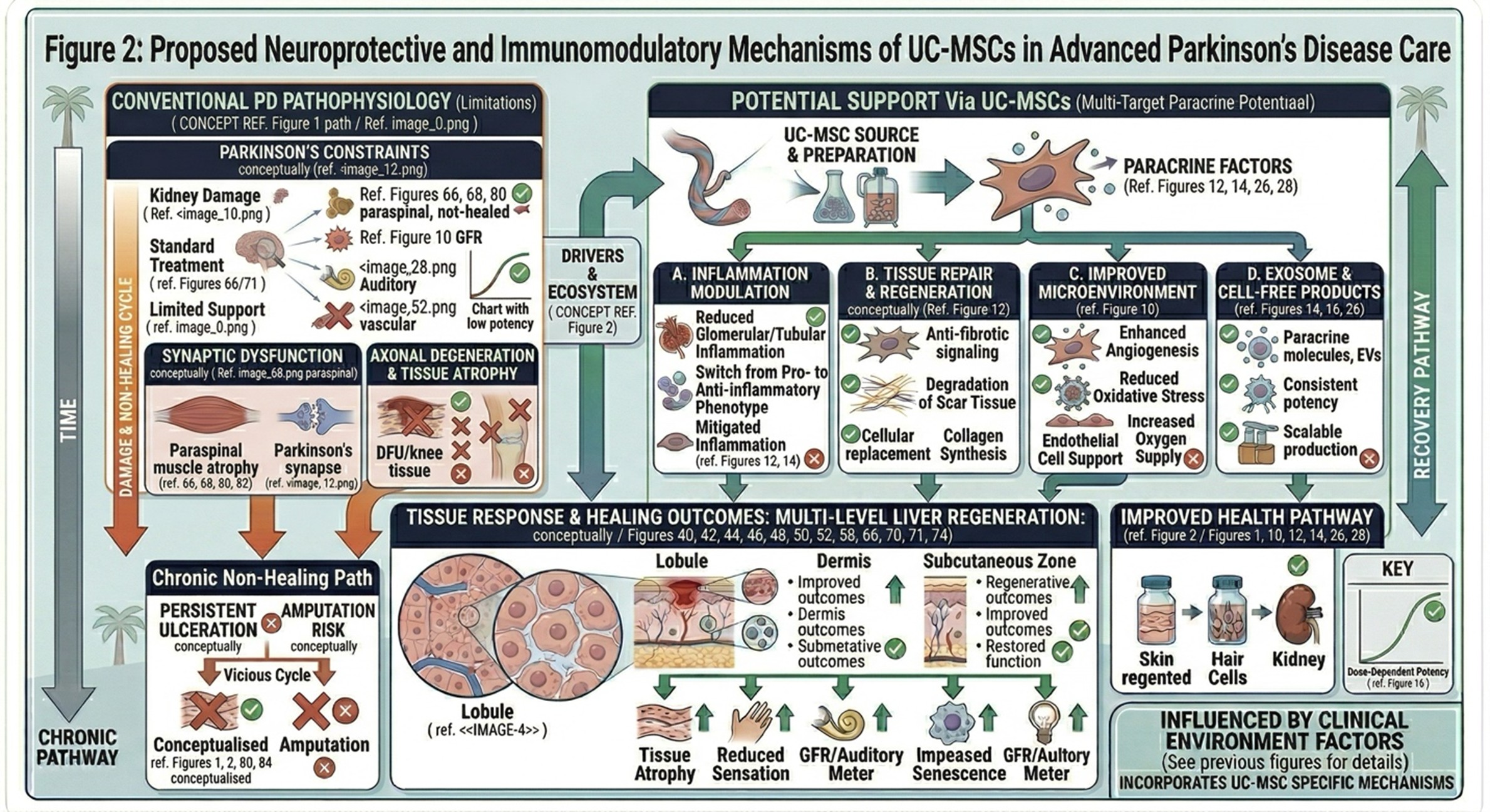
Against this backdrop, stem cell-based therapy is generating growing interest as a next-generation approach in the management of Parkinson’s. Instead of only replacing lost neurotransmitters, regenerative medicine aims to modulate the underlying neural environment so as to potentially shield vulnerable cells from losing their hyperactive counterparts and enhance tissue signaling that supports communication among survivor cells. Of the cell types currently being investigated, umbilical cord-derived mesenchymal stem cells (UC-MSCs) have gained particular importance due to their low immunogenicity, robust proliferative capacity and biologically active secretory profile.
UC-MSCs are not commonly discussed as naive cell replacement. Instead, they pique much of their therapeutic interest due to their capacity for modulating inflammation and releasing trophic factors as well as altering the microenvironment surrounding injured neural tissue. This broader biological influence finds more importance in Parkinson’s disease, which has multiple damaging pathways simultaneously operating. The idea is not just temporary symptom relief but creating a more stable and protective neural environment.
- Mechanistic Basis of UC-MSC Activity in Parkinson’s Disease
The therapeutic potential of UC-MSCs in Parkinson′ disease relies on a number of linked biological mechanisms.
Neurotrophic Support Through Paracrine Signaling
UC-MSC has known primarily to perform via paracrine action, i.e. UC-MSC releases bioactive and/or signaling molecules or factors that can affect adjacent or nearby tissue. It may support neuronal viability, synaptic integrity and functional resilience24; including neurotrophic factors like BDNFand NGF. Such a mechanism of trophic support may not only defend stressed neurons, but also increase local intercellular communication across the matrix of an injured or disease-afflicted brain.
Immunomodulatory Effects
Chronic neuroinflammation has now been acknowledged as a significant contributor to the pathogenesis of Parkinson’s disease. UC-MSCs have been investigated for their ability to modulate immune signaling in the CNS, and nasal UC-MSCs can even temper microglial activation. These cells may attenuate secondary injury due to inflammatory cytokines and glial overactivation by shifting inflammatory activity away from a pathologically perpetuating state.
Reduction of Oxidative Stress
Oxidative damage is another key contributor to neuronal loss in Parkinson’s disease. Methodologically, UC-MSC-derived signaling may increase endogenous antioxidant defenses and lower the burden of reactive oxygen species thereby enriching dopaminergic neuron protection from both apoptosis and cellular exhaustion.
Possible Neural Differentiation Potential
While paracrine and immunomodulatory effects are most widely discussed in the literature as current excite of mesenchymal stem cell-induced neurological recovery, there is also some hypothesis-driven works whether mesenchimal stem cells have a degeneration state as neuron-like or indirectly could support neural lineage repair under specific microenvironment conditions. It is still an evolving area of research and should be taken with a grain of salt, but it has further fueled scientific curiosity surrounding their greater regenerative potential.
- Regenerative Medicine Development in Thailand
Thailand is now a hub in the wide field of regenerative medicine and increasingly investing in biotechnology infrastructure, laboratory capability, and clinical translation. The country has been of particular interest to patients seeking advanced supportive therapies due to its combination of medical sophistication, treatment availability and growing experience in cell-based therapies.
Interest in Thailand, in the context of Parkinson’s disease, is related not only to clinical care but also to structured regenerative programs within laboratories processing and regulatory oversight. Such environment has inspired additional exploration of applications based on UC-MSC, especially clinical instances whereby traditional neurology might only provide symptomatic management but little in the way of restorative capabilities. With ongoing research efforts, we expect that Thailand will continue to play an active role in the establishment of ethically guided and scientifically based regenerative therapies.
- Concluding Perspective
The evolution away from symptom-based management toward biologically targeted neurorestorative care reflects a significant advancement in the treatment of Parkinson’s disease. While established therapies, such as levodopa and deep brain stimulation, remain important tools, their shortcomings reflect the need for strategies that can directly target the mechanisms of neurodegeneration. Under these changing circumstances, UC-MSCs are studied based on their possible effects of neurotrophic support, inflammation regulation, oxidative injury mitigation and neural microenvironment optimization. These characteristics make them an interesting subject of study in advanced Parkinson’s care. Responsible interpretation goes hand in hand: UC-MSC-based therapy should be framed as a supportive regenerative approach under active clinical investigation rather than a one-stop cure.
As regenerative medicine matures, bringing together timely cell-based intervention with conventional neurological management may be more complete in terms of supporting function, quality of life and long-term disease outcomes in Parkinson’s disease.