

Metabolic diseases continue to become increasingly prevalent on a global scale, with diabetes condition being one of the most devastating conditions in this group. Its most severe complications include the formation of chronic wounds, in particular diabetic foot ulcers that do not heal over time. These wounds can evolve into deep infection, threatening limb viability and significantly diminishing mobility, self-sufficiency and quality of life for a patient. In advanced cases, this could be the end result of amputation. Due to the inability of conventional treatments to lead to satisfactory healing more and more attention has been drawn to regenerative medicine. UC-MSCs are specifically being investigated for their potential in promoting tissue repair in diabetic wounds that exhibit chronic inflammation, impaired circulation, and healing. It has increased interest in diabetic wound healing stem cell therapy in Thailand.
- Why diabetic wounds develop and why they matter so much
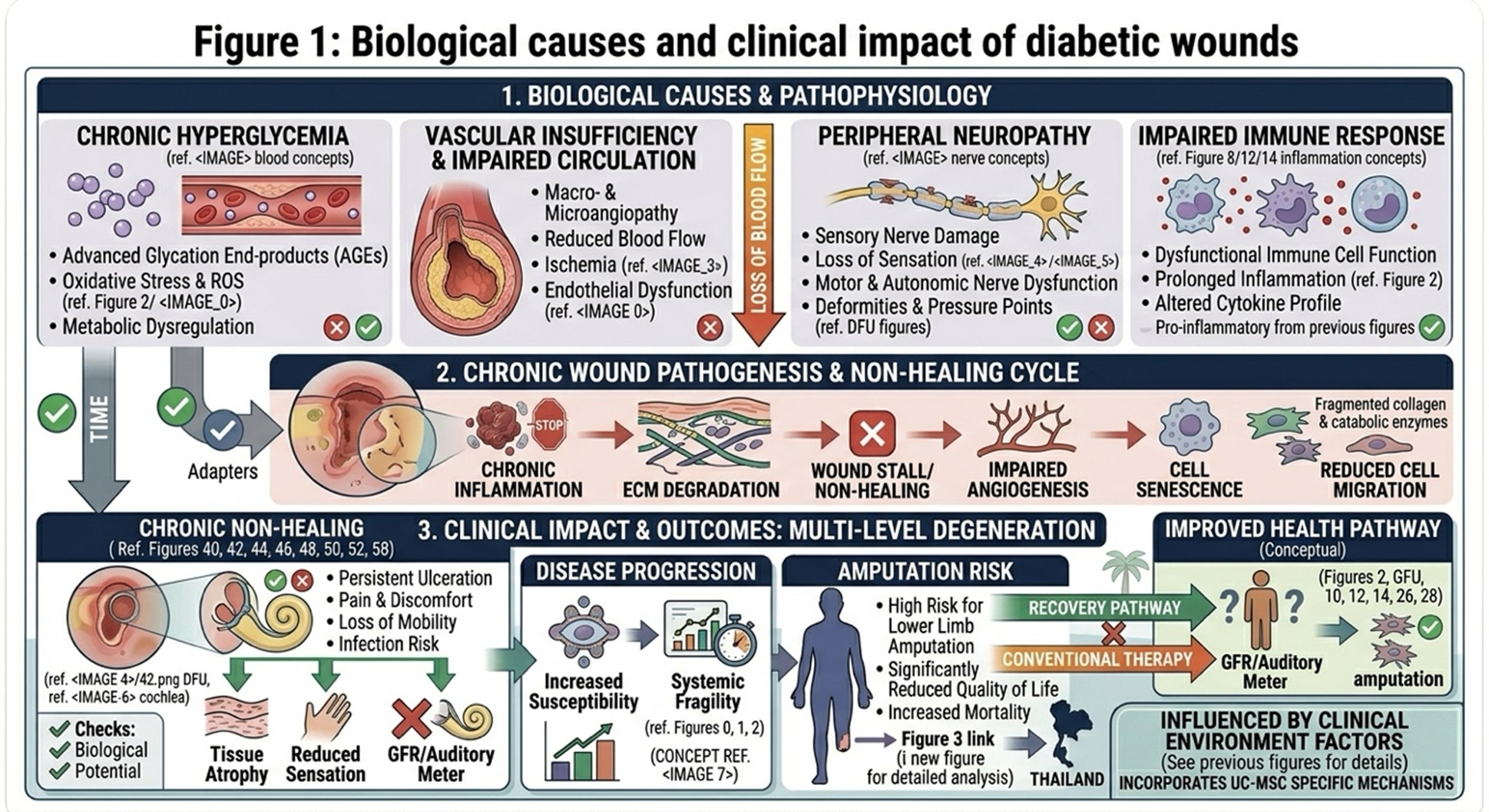
One reason diabetic ulcers are so hard to treat is that diabetes disrupts the ordinary healing response. In healthy circumstances, wound healing occurs through four overlapping phases, hemostasis, inflammation, proliferation and remodeling. But in diabetes, this process is frequently delayed or disrupted. Chronic hyperglycemia leads to overproduction of reactive oxygen species and advanced glycation end-products that aggravate cell stress, leading to tissue damage.
Consequently, the inflammatory phase of wound healing is prolonged. The wound remains in a chronic pro-inflammatory state instead of migrating forward into tissue repair and regeneration due to persistently elevated levels of pro-inflammatory cytokines such as TNF-α and IL-1β. Simultaneously, the formation of blood vessels is diminished, restricting oxygen and nutrient transport to the damaged zone. The reduced blood flow can result in tissue ischemia, necrosis and an increased risk of infection even with hard-to-treat bacteria. These compounding issues can make diabetic wounds not only slow to heal, but also hazardous to the patient’s long-term health and daily life.
- Conventional treatment approaches and their limitations
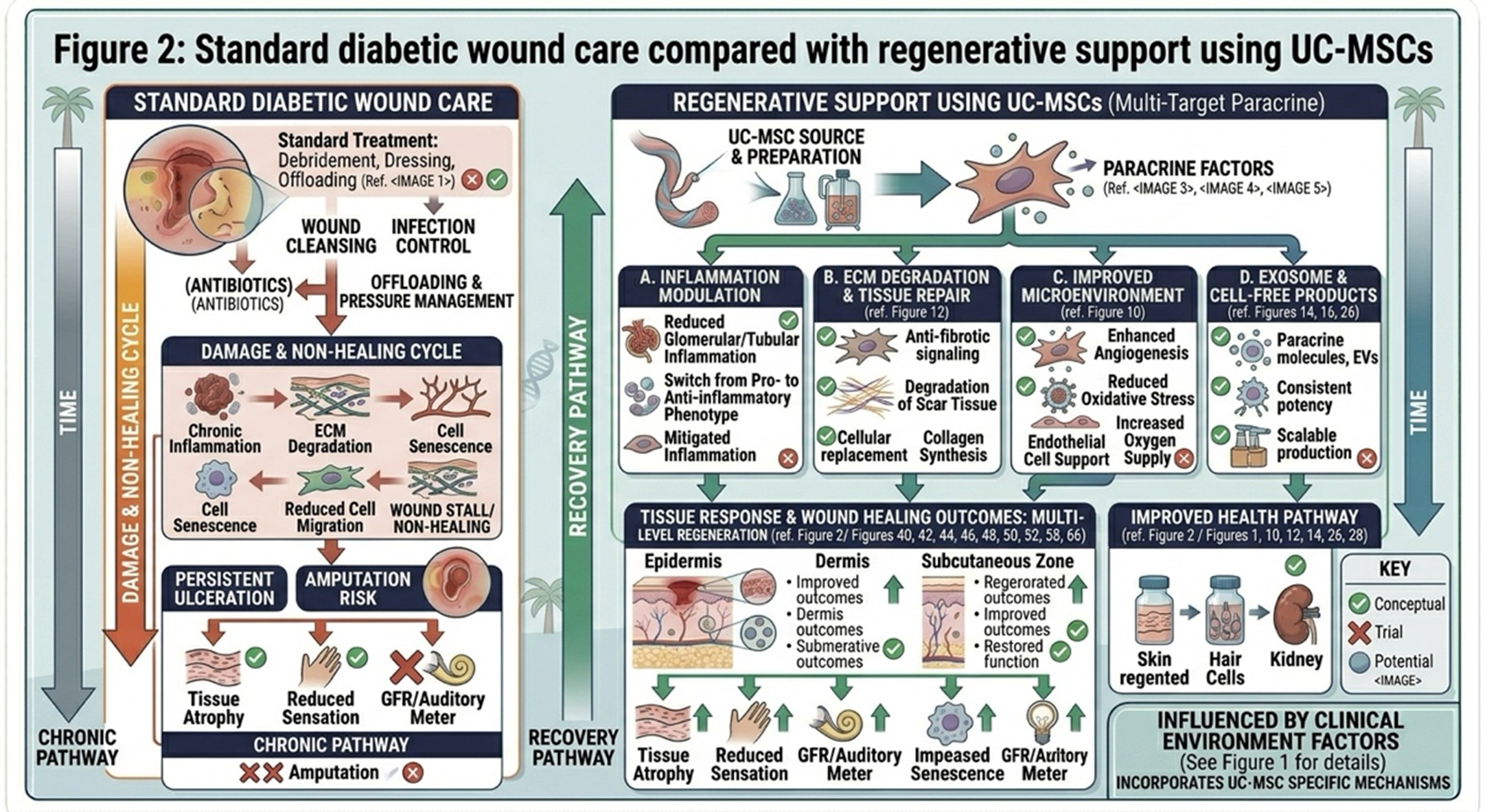
The modern standard of care for diabetic wound treatment is founded on cleaning the wound, debridement of necrotic tissue, off-loading to decrease pressure over the ulcer and dressings that keep a moist environment conducive for healing. These approaches are critical and continue to be the bedrock of care. They also assist in establishing a cleaner wound bed, minimizing some physical impediments to healing.
But traditional treatment often addresses only the surface of the wound in terms of appearance, and does less to address deeper biological issues that impede healing. Despite routine care for months to years in many patients, the wound environment continues to be depleted, poorly perfused, and biologically inactive. And in the case of a significantly compromised local cellular environment, growth factors and advanced dressings can only serve as bridging therapy. This is exactly why certain ulcers remain for months, or even years. A drawback of traditional wound care is that it tends to manage the wound without complete restoration of the compromised healing system beneath.
- Why UC-MSCs are attracting attention
This fact has gained special interest for the UC-MSCs due to their high proliferative capacity and their potential impact on the immune response and local tissue repair. In chronic diabetic ulcers, these cells are appreciated not merely as replacement cells but as biologically active mediators releasing a plethora of paracrine factors. These include molecules associated with growth such as transformative growth factor-beta and vascular endothelial growth factor, the latter likely involved in tissue regeneration and blood vessel sprouting.
In a pragmatic sense, UC-MSCs may assist diabetic wounds in two principal ways. First, they might dampen harmful inflammation by promoting a transition of macrophages from a pro-inflammatory state to a more reparative state. Second, they may support angiogenesis and restore blood flow to ischemic tissues. UC-MSCs may also promote fibroblast migration and collagen organization through regulating the wound microenvironment, which are critical for tissue structure reconstruction. This is at least one reason that diabetic wound healing stem cell therapy in Thailand has attracted more and more attention as a regenerative strategy for challenging, nonhealing ulcers.
compared with regenerative support using UC-MSCs
- Thailand’s growing role in regenerative wound care
Thailand has been increasingly becoming a key location for regenerative medicine. The nation has invested in high-level laboratory systems, clinical infrastructure and treatment pathways that facilitate cellular therapy deployment for complex conditions like diabetic complications. This led to the creation of a treatment context where personalized regenerative care can be embedded into comprehensive diabetes care.
Thailand’s advances in the arena of diabetic wound care is a reflection not only on laboratory capabilities, but also on having ample clinical experience. The combination of sophisticated cell-processing systems and customized wound-care protocols has made stem cell therapy a visible segment of the country’s regenerative medicine landscape. This may provide a pathway to more advanced biologic support for those with ulcers that fail to heal through standard methods alone.
- Looking ahead: from wound management to biological restoration
The next generation of diabetic wound care will go beyond merely managing symptoms and treating the outer layer of wounds. Because of this, regenerative medicine is growing a desire to heal the inner problems that go deep within our bodies: inflammation, poor blood supply and dysfunctional cells. There has been interest in exploring UC-MSCs as they may help to overcome some of these barriers, particularly within chronic wounds that have become recalcitrant to conventional care.
This is especially critical in diabetic foot ulcers, where delayed healing may result in partial or complete limb amputation. From a medical standpoint, that means some of the most meaningful goals of treatment are tissue preservation, maintaining mobility, and preventing amputation. The advancements in regenerative wound care and practice of Thailand imply that the stem cell therapy may be an integral component in future management of diabetic wounds. These therapies may help protect not only physical health, but also preserve dignity, function, and quality of life for people living with diabetes by enhancing healing potential and minimizing the risk of severe limb loss.