

Why does this keyword need a careful explanation
- “Plant-Based Stem Cell Therapy” sounds futuristic, but diabetes biology is more demanding than the phrase suggests
Those who search for Plant-Based Stem Cell Therapy for diabetes are invariably looking beyond blood sugar control. They are looking for restoration. That threat instinct works because diabetes is not merely about high glucose. In type 1 diabetes, the immune system attacks and kills insulin-producing beta cells in the pancreas. Metabolic control is progressively disrupted by the combined effects of insulin resistance and beta-cell dysfunction in type 2 diabetes. Both approaches come down to the same underlying question lurking behind the search: can pancreatic function be meaningfully rebuilt, protected, or replaced?
But the issue, you see, is that Plant-Based Stem Cell Therapy does not have a classic therapeutic category within conventional diabetes management. For the vast majority of use in real life, this phrase typically refers to either plant-based components that may theoretically promote metabolism or marketing language appropriating and much abused term “stem cell,” but not actually describing what constitutes a true cell therapy. That distinction matters because while serious diabetes regeneration research really is real, it does not consist of a plant supplement with sci-fi packaging.
What “Plant-Based Stem Cell Therapy” usually means in practice
- Most of the plant-based science in diabetes is about metabolic support, not transplantable stem cells.
The most credible plant-based literature in diabetes focuses on dietary patterns, phytochemicals, and natural compounds that may improve insulin sensitivity, oxidative stress, inflammation, or beta-cell stress. A 2024 review in Nutrients describes plant-based diets and phytochemicals as potentially helpful in diabetes management through mechanisms such as better glycemic control, improved insulin sensitivity, and modulation of metabolic pathways. That is scientifically interesting. But it is still very different from a proven regenerative therapy that rebuilds the pancreas.
This is where a lot of online writing becomes slippery. A compound can have useful biological effects without becoming a true stem-cell treatment. Some plant-derived molecules may help create a healthier metabolic environment, and some may even protect pancreatic function in preclinical work. But that does not mean Plant-Based Stem Cell Therapy has become an accepted medical pathway for diabetes treatment. It means nutrition and phytochemistry are being studied as supportive tools inside a much larger metabolic story.
- “Stem cell” on a product label is not the same thing as real regenerative medicine.
It is a point that regulators have been pretty blunt about. According to Singapore’s Health Sciences Authority, claims that live stem cells are found in oral supplements are false and scientifically implausible, considering that viable stem cells must be stored at temperatures below-196 °C, so they would never survive the digestive tract. That is a not-as-closely-hitched reminder that supplements can feel regenerative, do fine-tuned as true essentially ever sense substantive. That matters a great deal for an audience with diabetes, because the hope that pancreatic repair will become possible is genuine enough to make misleading words particularly convincing.
Where real stem cell pancreas regeneration research actually stands
- This field is real, and it is much more serious than the marketing around it
The phrase stem cell pancreas regeneration points to one of the most active and difficult frontiers in diabetes science. Broadly, the field has two major directions. One is exogenous replacement: producing insulin-secreting beta-like cells or islets from stem cells and transplanting them into patients. The other is endogenous regeneration: trying to stimulate the pancreas itself to regenerate or expand beta-cell mass through replication, reprogramming, or neogenesis. Recent reviews describe both strategies as scientifically promising, but also emphasize that translation remains difficult.
That distinction gives the topic its first real layer. When people hear “pancreas regeneration,” they often imagine one direct solution. In reality, the field is split between replacing lost function from the outside and trying to recover it from within. Both are exciting. Neither is simple.
- The most advanced human evidence is in stem-cell-derived islet replacement.
This is the component of the story that has progressed farthest from theory. Reporting in Nature Biotechnology (2024), encapsulated, stem cell-derived beta cells can regulate glucose levels in subjects with type 1 diabetes. Fast forward to 2025, and a NEJM study in the area of stem cell-derived islets that were fully differentiated showed engraftment with endogenous insulin production and physiologic restoration of islet function in subjects with type 1 diabetes. The significance of those results lies in the fact that cell-based replacement is no longer a mere laboratory ambition. Now it’s generating useful human signals.
But the science still needs to read the science with discipline. And these studies do not mean diabetes has been resolved or that every regenerative claim is established medicine. Current work has the most strength in carefully selected patients and continues to combat significant hurdles related to immune protection, graft survival, implantation biology, manufacturing consistency, and long-term durability. Several initiatives, including those associated with the Human Islet Research Network and recently founded programs to investigate loss of beta-cell function in diabetes research, have characterized remaining major knowledge gaps around restoration of protection/destruction/differentiation.
Why is endogenous pancreas regeneration so appealing, and so hard
- Rebuilding beta-cell mass from within is one of the most attractive ideas in diabetes science
While exogenous replacement is the engineering route, endogenous regeneration can be conceived as a biological dream. For example, a 2024 Trends in Endocrinology & Metabolism review calls beta-cell regeneration “an appealing pathway to diabetes treatment,” but also cautions that making it clinically realizable has proven challenging. A review on beta-cell replication published in 2025 reiterated this message: steps forward had surely been made towards both understanding how the concept of expansion by outcome could be understood through a model known as RETI (replication, exocytosis and trans differentiation integration), but obstacles exist before these insights become safe therapies for humans.
This is important because it helps put Plant-Based Stem Cell Therapy in the right place. Plant compounds may eventually help support metabolic health or influence some of the signaling pathways relevant to pancreatic stress. But true stem cell pancreas regeneration is operating at a much deeper level of biology and is still being built through rigorous experimental and clinical work, not through simplified retail language.
The most honest way to connect these ideas
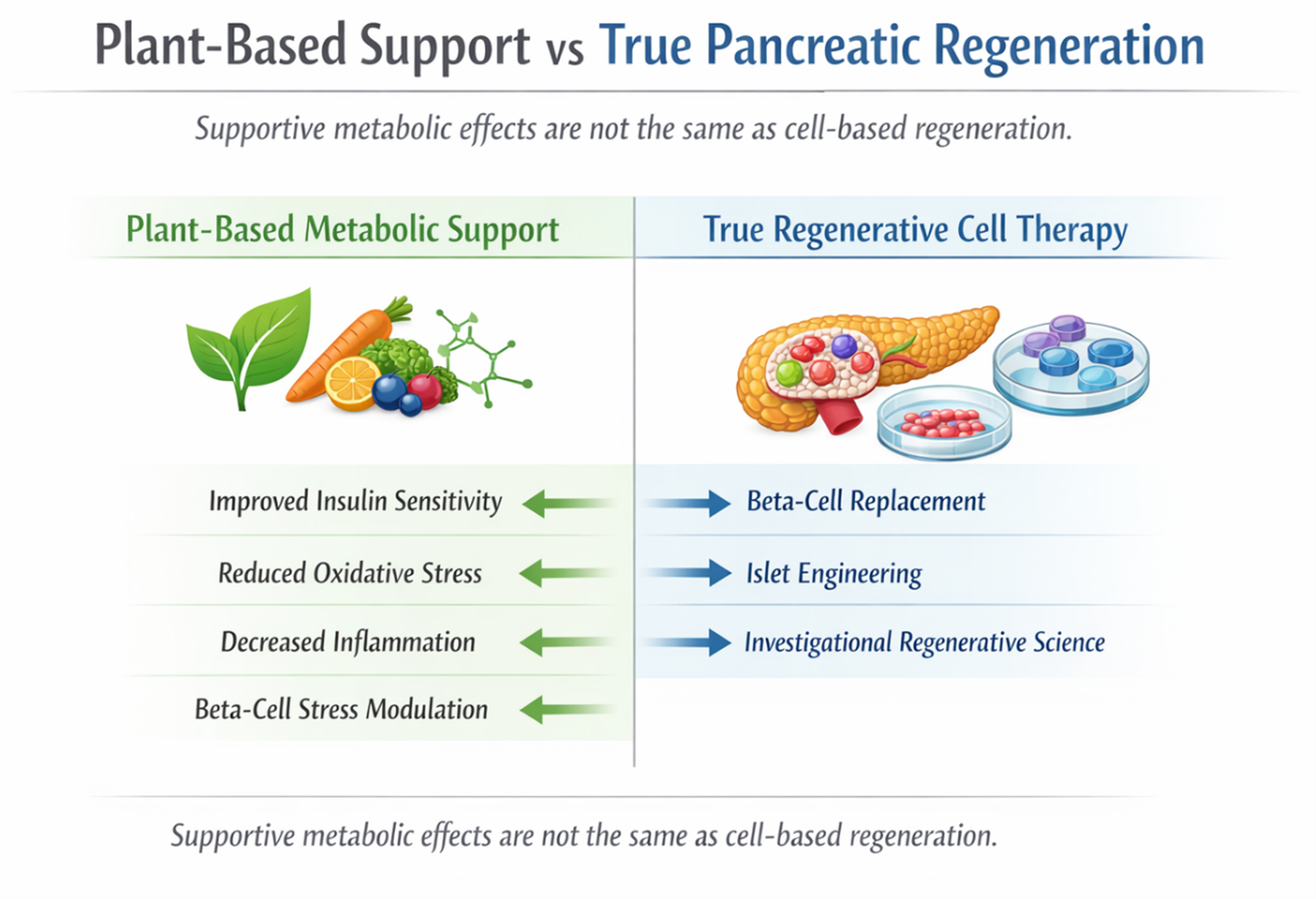
- Plant-based support and stem-cell regeneration are not the same tier of intervention.
The most useful way to explain this topic is probably the simplest one. Plant-based strategies may matter in diabetes because diet quality and phytochemicals can influence insulin sensitivity, oxidative stress, and inflammatory tone. Stem-cell-based pancreas regeneration matters because it aims to restore lost beta-cell function more directly. Both belong in the diabetes conversation, but they do not belong on the same rung of the ladder. One is mainly supportive and metabolic. The other is genuinely regenerative and still largely investigational.
- The honest conclusion
If somebody is looking for Plant-Based Stem Cell Therapy for diabetes, then the most honest answer today is that this phrase is more SEO than a proper medical category. Actual beta-cell replacement, islet engineering, and endogenous pancreas-regeneration research (the real regenerative science) are more closely tied to personal meaning-related issues than restoration didactic ones. Framed not as a path toward rapid pancreatic rejuvenation, but rather as touch-up metabolic assistance or local support of compositional health, the plant-based subplot becomes the more credible partner. That does not mean that it is unimportant. It simply means the evidence must be put together properly.
In the end, the most powerful part of diabetes care is still often the least dramatic: looking after the body early, consistently, and seriously. Even when regenerative science is advancing, blood sugar control, nutrition quality, movement, sleep, and regular medical follow-up still matter enormously. Sometimes the most hopeful thing is not chasing the loudest promise, but giving your health the kind of steady care that makes every future option more meaningful.