

- Introduction to Neurodevelopmental Challenges
Neural connectivity, synaptic signaling, immune balance and sensory integration are all highly tuned processes that shape the developing human brain. In the case of Autism Spectrum Disorder (ASD), these processes could develop in a way that differs and leads to more diversity in communication, behavior, social interaction and sensory processing. ASD is not a single disease with one cause and one solution. It is a spectrum with different biological and developmental presentations.
Families frequently describe language delays, repetitive behaviors/social quirks, emotional dysregulation, sensory issues and difficulty tolerating change. Standard care remains behavioral, developmental and educational including speech therapy, occupational therapy and behavioral interventions such as ABA. These are still the pillars of autism care.
In parallel with the latter advances in research, an interest in biological pathways may be involved in symptoms among cases may develop over which the former are reversed that include neuroinflammation, oxidative stress and dysregulated synaptic signaling. This particularly has driven some interest in umbilical cord-derived mesenchymal stem cells (UC-MSCs) and curated brain-supportive or “brain booster” interventions as potential adjunctive medical interventions. Early results look promising, but these strategies are investigational rather than established cures.
- Biological Mechanisms in Autism
More recently, research has indicated that certain individuals with ASD may develop signs of immune dysregulation, microglial activation, oxidative stress and imbalanced neural circuits. These discoveries do not apply to every patient, but they help clarify why some researchers are investigating therapies intended to sustain the brain’s internal milieu, and not merely outward behaviors.
Microglia are the brain’s own immune cells. Deregulated microglial activity, in turn, can affect inflammatory signaling that impacts synaptic communication and neural plasticity. Also, oxidative stress and mitochondrial dysfunction have been mentioned as possible contributors in selected cases in the ASD literature.
This biological understanding has stimulated interest in therapies which could modulate inflammation, enhance neuronal signaling and promote the local milieu facilitating brain function. This does not imply that every autistic person needs biological treatment, but it does explain why regenerative and neuro-supportive strategies are receiving more serious attention than ever before.
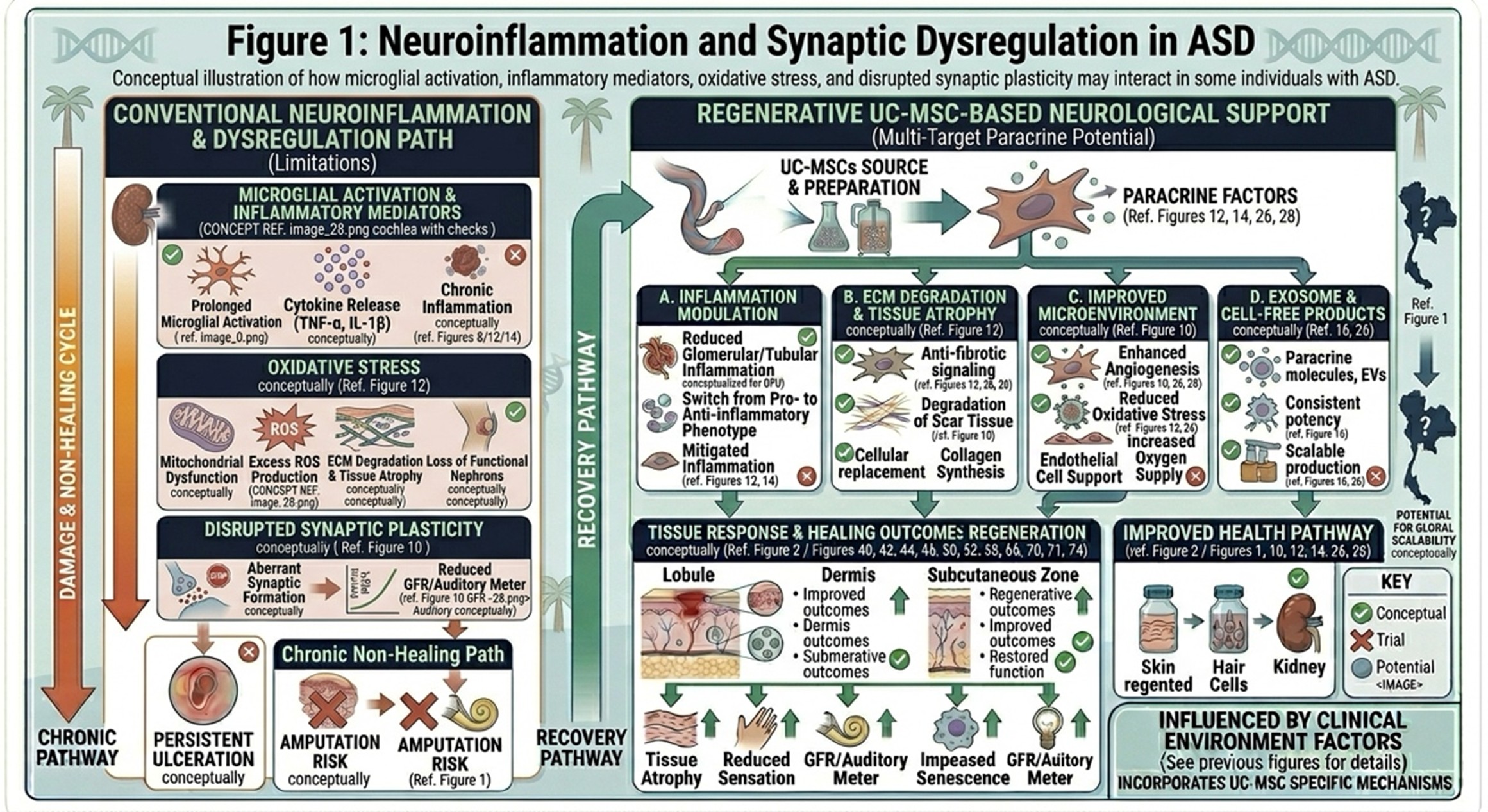
Conceptual illustration of how microglial activation, inflammatory mediators, oxidative stress, and disrupted synaptic plasticity may interact in some individuals with ASD.
- Limits of Conventional Approaches Alone
Traditional autism treatment is a valuable, evidence-based approach, but it has real-world limits. Behavioral and developmental therapies improve communication, self-regulation, daily function and learning outcomes but do not specifically act on underlying biological pathways that may be active in certain patients.
Medication can also be given to target related symptoms, like irritability, anxiety, sleep problems or attention difficulties, but again this is usually about symptom management rather than biological repair. For some families, progress is meaningful but slow, which explains why there is growing interest in supportive strategies that could help complement — not replace — standard therapies.
A more balanced message is not that conventional care is insufficient, but rather that autism treatment may someday be integrated less into an overall process. Behavioral therapy helps build skills. Medical and biological strategies might, in select cases, help optimize the environment within which those skills are taught and deployed.
- Potential Benefits of UC-MSCs in Autism Support
Since mesenchymal stem cells secrete signaling molecules (cytokines, growth factors and extracellular vesicles) potentially regulating immune balance, inflammation and cell-to-cell communication, UC-MSCs are being studied. In the context of autism research, it’s not so much that these cells are likely to directly take on a role as neurons, they may help regulate their environment around existing network.
Preclinical and early clinical work has reported potential benefit of such approaches on some patients in social interaction, communication, and behavioral regulation. A few reports and reviews have also shown good short-term safety profiles in research settings, but the authors stress overall that larger high-quality trials are still needed to confirm efficacy, dosing, patient selection and long-term safety.
umbilical-derived MSCs have an advantage in accessibility, low immunogenicity and strong interest in its immunomodulatory profile. For clinics and families, though, the clear message should be caution: UC-MSCs are support investigational option but no cure for autism.
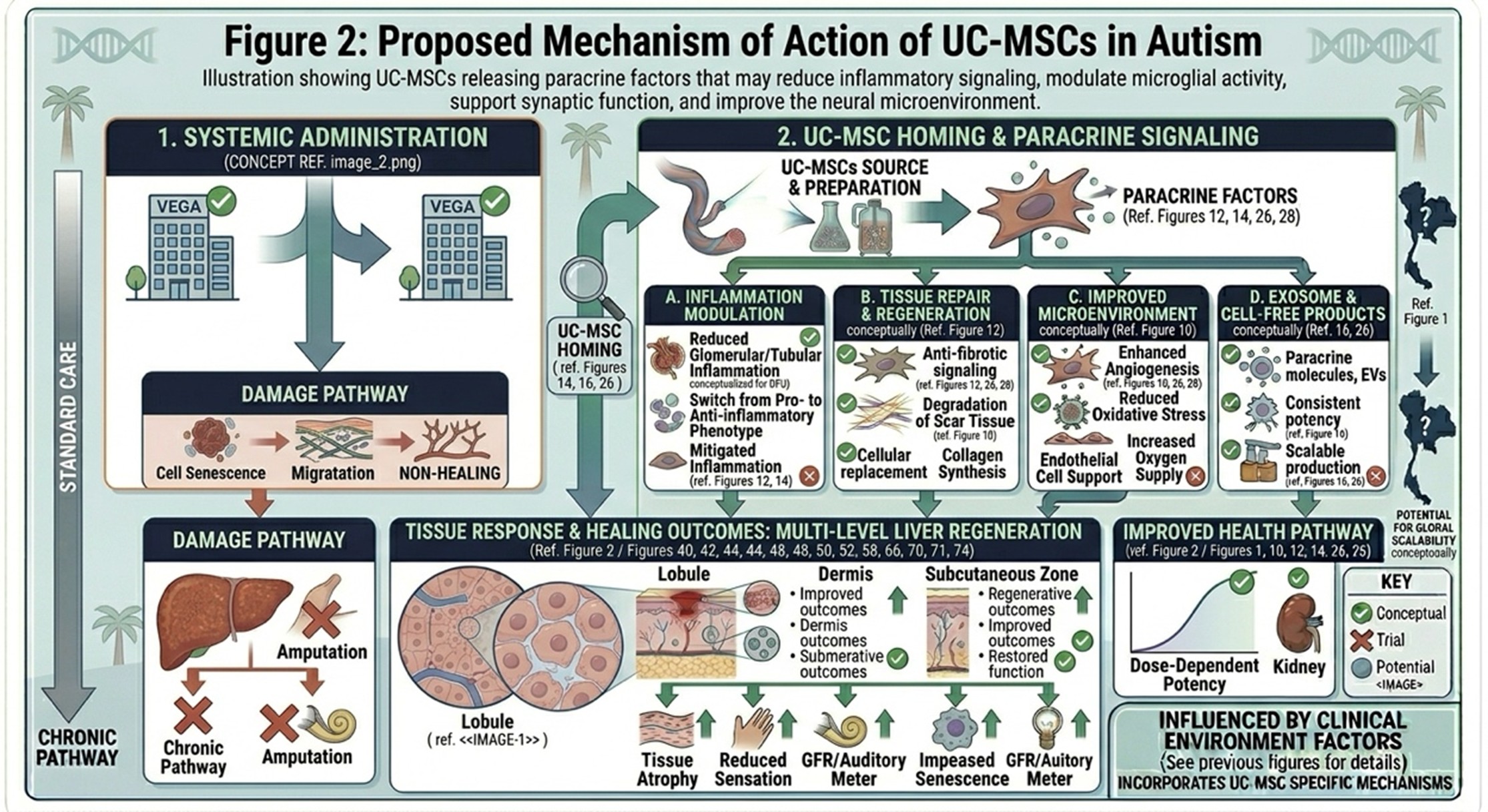
Illustration showing UC-MSCs releasing paracrine factors that may reduce inflammatory signaling, modulate microglial activity, support synaptic function, and improve the neural microenvironment.
- Brain Booster Strategies and Neuro-Supportive Peptides
The phrase “brain booster” can refer to vastly different things, so use it with caution. In a clinical or scientific context, it can refer to specific neuro-supportive compounds, peptide-based modalities, mitochondrial support or other such interventions, intended to facilitate neuronal signaling resilience and metabolic homeostasis. Because the evidence level is highly variable depending on the compounds in question, they should not all be clumped together and treated without distinction as if they have the same weight of evidence behind them.
There is a peptide-specific neuroprotection literature which describes potential mechanisms like decreased oxidative stress, restoration of mitochondrial function, synaptic plasticity modulation, and modulation of inflammatory pathways. These mechanisms are of biological interest, particularly in contexts where neuroinflammation and/or signaling imbalance are implicated. But for autism in particular, peptide-based approaches are still far less established than mainstream behavioral care, and the evidence supporting them is also still early or experimental in many instances.
That said, a more expanded notion of brain-supportive therapy jibes with a more contemporary view of autism care: Keep the brain working as effectively as possible while maintaining structured therapy and education and support for families. In practice, there should be a component of such a plan that is individualized, medically supervised and described honestly as adjunctive to definitive therapy.
- The Role of Specialized Medical Centers
In the face of growing interest in regenerative and neuro-supportive medicine, specialized centers are increasingly developing multidisciplinary programs that integrate medical evaluation consistent with developmental therapies and selected biologically targeted interventions. In autism care, this sort of center may lead pediatric evaluation to rehabilitation planning and supportive treatment selection in a more integrated way.
The benefit of a specialized clinic is not just the intervention, but the whole surrounding system: appropriate screening, realistic expectation-setting, safety monitoring and integration with ongoing speech, occupational, behavioral or education support. This matters because rarely does an autism outcome depend on one therapy alone.
Down the road, we hope to have better biomarkers, better subgroup selection, and stronger clinical trials that will help us define which individuals may be most likely to benefit from adjunctive biological therapies like UC-MSCs or selected brain-supportive compounds. Currently, specialized care will need to balance the appropriate selection of candidates with responsible messaging.
- Final Thoughts on Supportive Care in Autism
Autism is complex, lifelong and highly individual. There is no one-size-fits-all intervention for every patient. Traditional therapies continue to be valuable, but increasing research into neuroinflammation, immune signaling, oxidative stress and neural plasticity has made new supportive strategies a possibility. Because of their immunomodulatory and paracrine properties, UC-MSCs are being investigated, and both early results show potential for supportive effects in selected cases. Similar brain-supportive or peptide-oriented strategies may emerge in the future toward promoting a better neural environment, though the evidence is mixed and intervention-specific. These should not be portrayed as guaranteed or curative options.