

A different way to think about diabetic foot ulcers
Diabetic foot ulcers are not mere “skin wounds. They often develop in a setting of neuropathy, diminished circulation, repetitive pressure, chronic inflammation and increased risk of infection. That combination is one reason that these ulcers can be persistent and challenging to close. International diabetic foot guidelines currently remain focused primarily on structured wound care measures: debridement, offloading, vascular assessment and revascularization when indicated as well as infection management when necessary. Advanced biologics should be considered adjunctive therapy to this foundation, rather than an alternative to it.
Where a UC-MSC stem cell clinic fits in
Consequently, a UC-MSC stem cell clinic is optimally positioned to serve as an investigational service resource for those with difficult-to-heal wounds. UC-MSCs are being studied for their potential to modulate the wound environment via paracrine signaling, inflammatory modulation, and promoting angiogenesis and tissue repair. Recent reviews still characterize MSC-based therapy for diabetic wounds as promising, but they note that the field remains maturing and insist that larger, better standardized studies are required before unequivocal standards of care can be proclaimed.
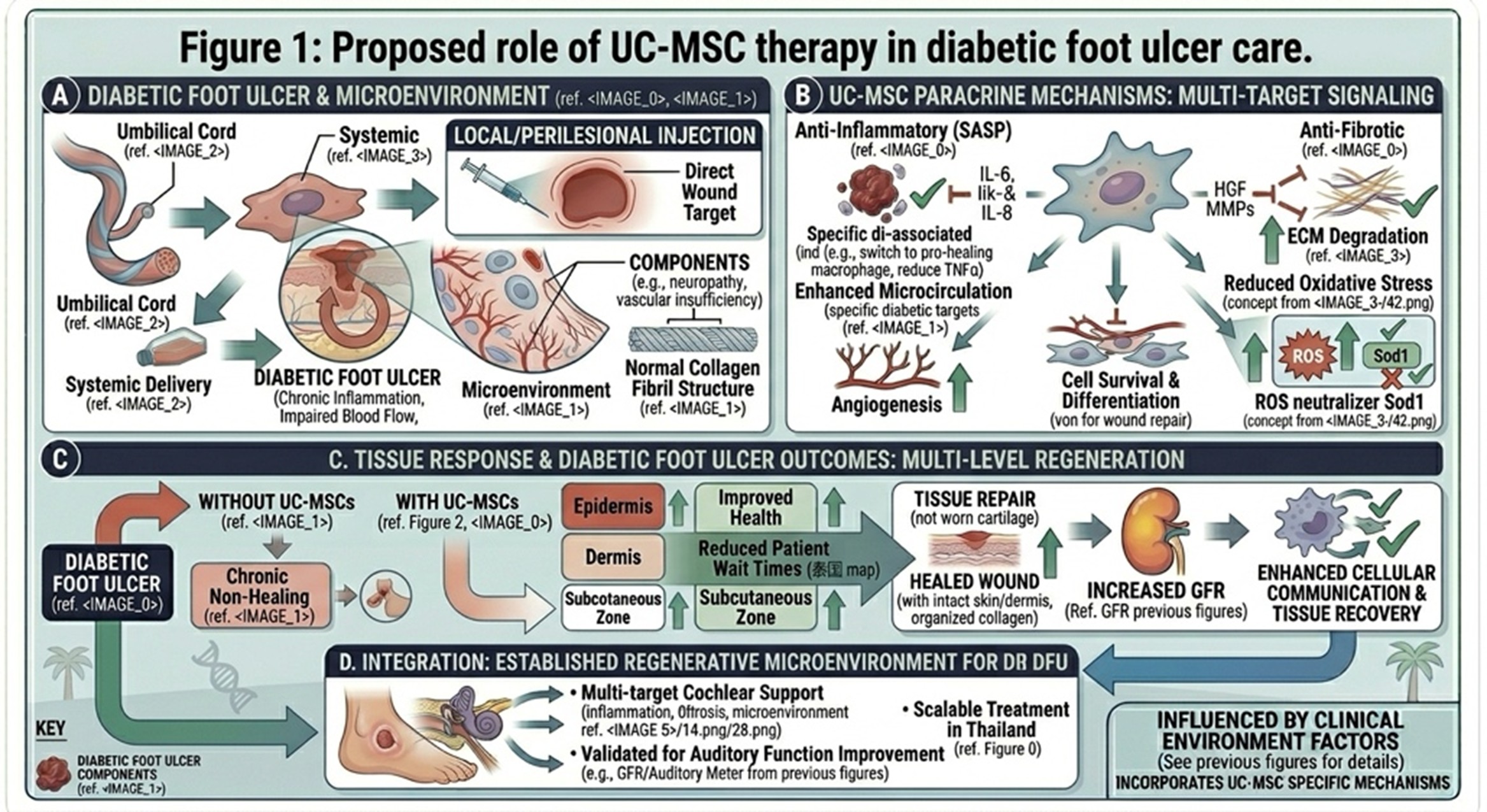
Standard diabetic foot management remains the base layer of treatment, including debridement, offloading, glucose control, infection management, and vascular assessment. UC-MSC-based therapy is being investigated as a regenerative adjunct that may support wound healing through anti-inflammatory, angiogenic, and tissue-supportive signaling.
Topical treatment is another direction worth noting
Another, more recent study altered this model even further: instead of injected whole-cell UC-MSCs, they employed topical delivery. In the 2024 phase 1 trial of an allogeneic umbilical cord lining MSC product, treatment was administered via topical application twice weekly to a maximum of 8 weeks following debridement. No serious product-related adverse reactions were reported, and a significant reduction in ulcer area was observed. This doesn’t set routine clinical practice, but supports the broader point that wound-focused local delivery may be more relevant than giving cells the more common intravenous route.
What a responsible clinic article should still say clearly
An ideal stem cell clinic article can still be written showing that advanced regenerative treatment is not a substitute for basic diabetic foot care. Patients still require pressure relief, cleansing of the wound, debridement, optimization of blood sugar levels, treatment for infection if necessary and an assessment for any vascular issues. That message is important for trust and accuracy because traditional diabetic foot care remains the primary driver of good outcomes.
Regulatory reality
It should also be made clear that patients need to be wary of products marketed via the internet or heavily promoted.” In March 2026, the FDA once again cautioned patients and consumers not to use unapproved products made from human cells or tissues that were being advertised for a myriad of diseases and conditions,the FDA had not necessarily assessed their quality, safety, purity or potency. That is why UC-MSC therapy for diabetic foot ulcers should be termed investigationaland closely monitored, not an established treatment.
Final summary
More modern and stronger way to present this topic could be: a UC-MSC stem cell clinic for diabetic foot ulcers may offer a regenerative adjunct for selected chronic wounds, with treatment atop standard piece of multidisciplinary wound care. The clearest whole-cell usage protocol is a practical one of 10 million cells per treatment in adults over the weight of 50 kg, typically given in three doses, with local wound-edge and wound-base injection being the most pertinent/commonly used wound-directed step, reserving IV support for selectively indicated ischemic cases. That framing is more therapeutic and SEO-friendly.