

Crohn disease is more than just tummy ache, diarrhea, or 1-time at the bathroom discomfort. IBD is a chronic and recurrent inflammatory bowel disease, characterized by abnormal immune regulation of gut microflora. In other patients, the inflammation remains toward the surface. In others, it may penetrate more deeply into the bowel wall resulting in ulceration, strictures, fistulae, abscesses, malnutrition, loss of strength and recurrent exacerbations.
Therefore stem cell therapy Thailand for Crohn’s Disease remains as a research interest. Patients are not only looking for relief from symptoms. A lot wants to know if the diseased gut and inflamed mucosal environment would be better covered biologically.
Equally careful lies a responsible discussion. Claiming UC-MSC stem cell therapy as a cure for Crohn’s disease or an alternative to gastrointestinal care is inadvisable. Currently, the most solid immune cell dialogue using stem cells is in carefully selected complex perianal fistulizing disease though general use for intestinal irritation and mucosal ulceration continues to be of broad clinical investigation.
Crohn’s Disease Begins at the Barrier
The intestinal barrier is a complex entity, not just a lining. This is composed of epithelial cells, mucus, immune cels, microbiome signals blood vessels, tight junctions and repair pathways separating the contents of the gut from deeper levels of tissue.
This barrier is frequently inflamed and disrupted in Crohn’s Disease. When the mucosa is damaged, bacteria and food antigens may have a stronger interaction with the intestine immune system. Thus, a vicious cycle of ulceration-immune activation-pain-diarrhoea-bleeding-dyscrasia might be established.
Restoration of the intestinal barrier represents more than just sealing a surface ulcer. It means nourishing the tissue milieu that helps the gut lining relax, heal and is protected.
Why Mucosal Ulceration Matters
Mucosal ulceration is clinically relevant as it indicates ongoing tissue damage. The patient’s complaint may worsen when the bowel lining remains ulcerative, yet pain seems to [temporarily] improve. Recurrent ulceration may also predispose you to complications, namely strictures (narrowing of the intestines), fistulae, anemia and weight loss.
While acute intervention tells us how far we need to go to alleviate symptoms of Crohn’s disease, modern management often sets its sights on deeper control than symptom improvement. Inflammatory markers, stool calprotectin, imaging, endoscopy, and mucosal healing may be monitored based on physician preference.
That is one of the reasons why regenerative medicine comes into play. It is not only whether or not symptoms feel better. But the more important question is if the tissue environment itself is on a repair trajectory.
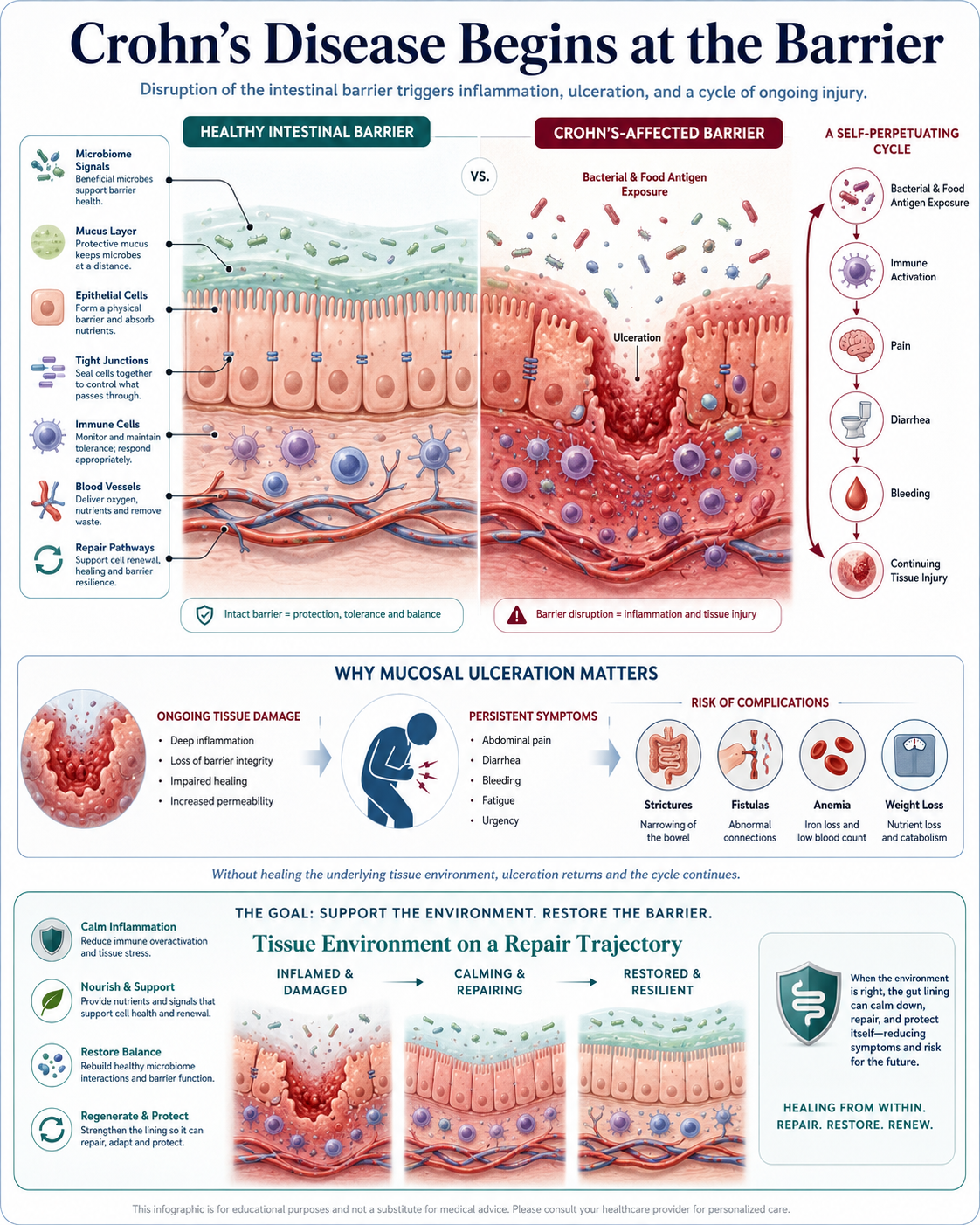
Figure 1: Stem Cell Therapy Thailand for Crohn’s Disease: Intestinal Barrier Repair and Mucosal Ulceration Support
How UC-MSC Stem Cell Are Being Studied
Umbilical cord-derived mesenchymal stem cells (UC-MSCs) are investigated for their biological behaviors including immunomodulation and paracrine signaling. Their primary interest is not that they evolve into new gut lining directly in a straightforward manner.
The reasonably prevailing mechanism is communication. UC-MSC stem cells also may release cytokines, growth factors, other bioactive molecules such as extracellular vesicles which affect immune behavior of immune cells and can stimulate inflammation resolution, impact oxidative stress response signaling attributes, angiogenesis and tissue reparative or regenerative signals.
This is significant as the disease in Crohn’s Disease exists and indicates immune imbalance and thus a disrupted mucosal environment. Use of UC-MSC stem cells signaling to facilitate a less inflammatory microenvironment better supportive of repair may merit exploration.
Intestinal Barrier Repair Is Not a Quick Patch
A leaky gut is not the same as sealing a hole with glue: you can’t just fill up gaps and expect it to be healed. This involves synergistic healing processes such as epithelial regeneration, immune homeostasis, blood supply restoration, microbiome stabilization and extracellular matrix remodeling with regulated inflammation.
It is conceivable if UC-MSC stem cells based support (not as mechanical patch, but biological signaling) This is intended to assist in modulating the local immune environment and to facilitate repair communication when the tissue remains inflamed and slow to heal.
But not every patient with Crohn’s is up for it, of course. Location and extent of the disease, presence or absence of fistulae, risk of infection, previous medical therapy, nutritional status and activity at presentation are all important.
The Strongest Evidence Is in Selected Fistulizing Crohn’s Disease
A leaky gut is not the same as sealing a hole with glue: you can’t just fill up gaps and expect it to be healed. This involves synergistic healing processes such as epithelial regeneration, immune homeostasis, blood supply restoration, microbiome stabilization and extracellular matrix remodeling with regulated inflammation.
It is conceivable if UC-MSC stem cells based support (not as mechanical patch, but biological signaling) This is intended to assist in modulating the local immune environment and to facilitate repair communication when the tissue remains inflamed and slow to heal.
But not every patient with Crohn’s is up for it, of course. Location and extent of the disease, presence or absence of fistulae, risk of infection, previous medical therapy, nutritional status and activity at presentation are all important.
Standard Crohn’s Care Still Comes First
Crohn’s Disease typically requires closely monitored gastroenterology management. Depending on the patient’s condition, standard treatment can consist of aminosalicylates in limited settings, corticosteroids to induce short-term control or maintain remission, immunomodulators such as azathioprine or mercaptopurine for maintaining remission, biologic agents including anti–tumor necrosis factor-α (anti-TNF-a) monoclonal antibodies, small molecules (e.g. tofacitinib), antibiotics (e.g. thiopurines) nutritional therapy and/or surgery or fistula-specific treatments.
Keep in mind that stem cell therapy is adjunctive and exploratory, not a substitute. Discontinuing Crohn’s medication without the guidance of a specialist can trigger severe flares or complications.
What a Responsible Program Should Assess
Before considering stem cell therapy Thailand for Crohn’s Disease, the medical team should review diagnosis history, disease location, colonoscopy findings, imaging, stool calprotectin, CRP, anemia status, albumin, nutritional markers, current medications, biologic history, infection screening, fistula or abscess history, prior surgery, and gastroenterologist notes.
Active abscess, uncontrolled infection, severe malnutrition, bowel obstruction, or urgent surgical complications require conventional medical care first.
Final Perspective
Targeting the intestinal barrier in Crohn’s Disease presents a complex challenge. It combines immune modulation, mucosal healing, balanced microbiome, tissue repair signaling and tightly controlled disease activity.
The UC-MSC stem cells paracrine signaling and immunomodulation has the potential to deliver a supportive regenerative conversation in selected patients, as demonstrated by clinical applications of stem cell therapy thailand. But to state it must be done with candor: potential research, strongest support in specific fistulizing Crohn’s, and not overall curative thing.
The golden path however still lies with integrated care: GI management and inflammation monitoring, nutrition, infection control, realistic expectations and regenerative support only if medically indicated.